Department of Medicine, Professorial Block, Queen Mary Hospital, Pokfulam Road, Hong Kong, China.
Shanghai Institute of Hematology, State Key Laboratory of Medical Genomics, National Research Center for Translational Medicine at Shanghai, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
J Hematol Oncol. 2022 Jun 3;15(1):74. doi: 10.1186/s13045-022-01293-5.
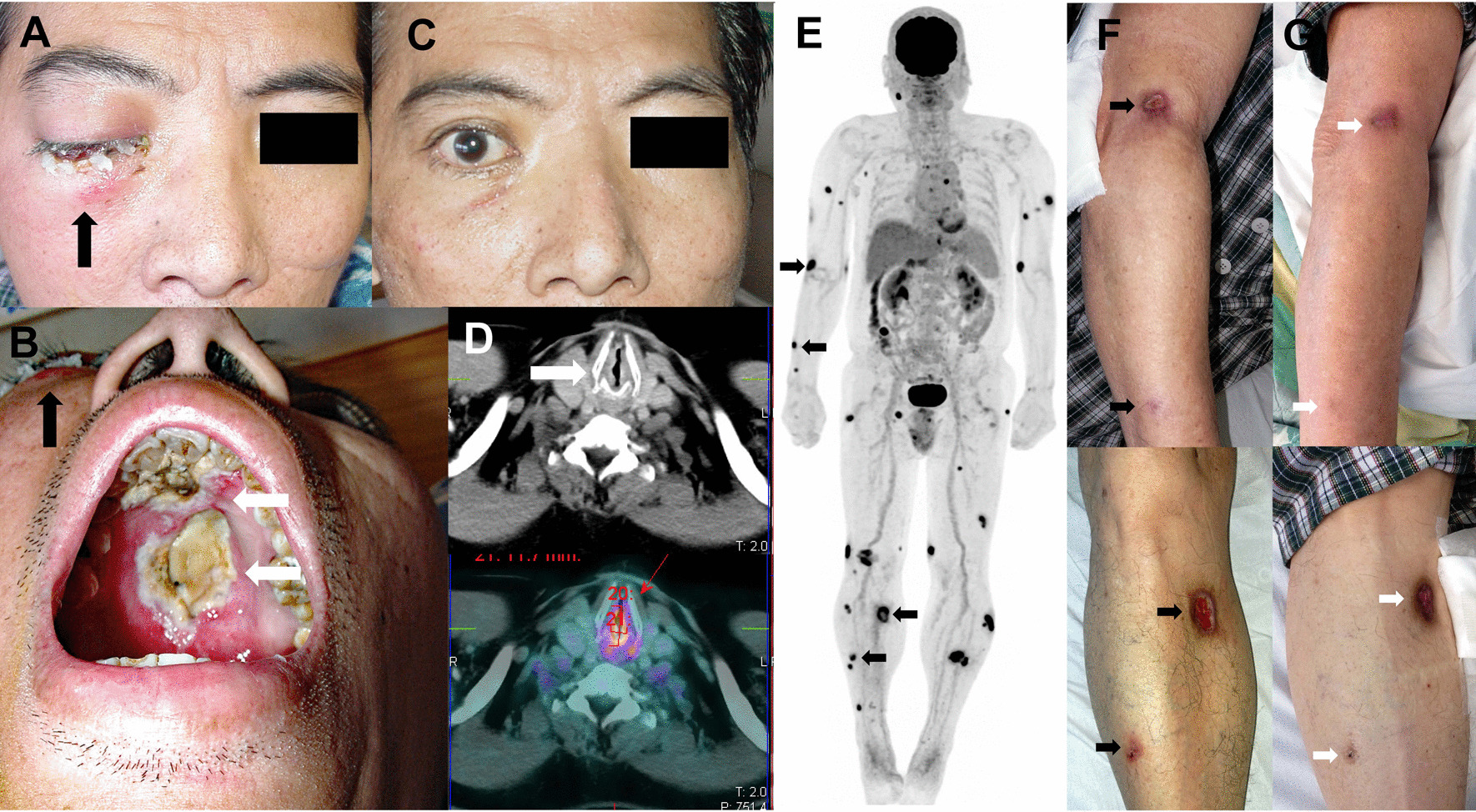
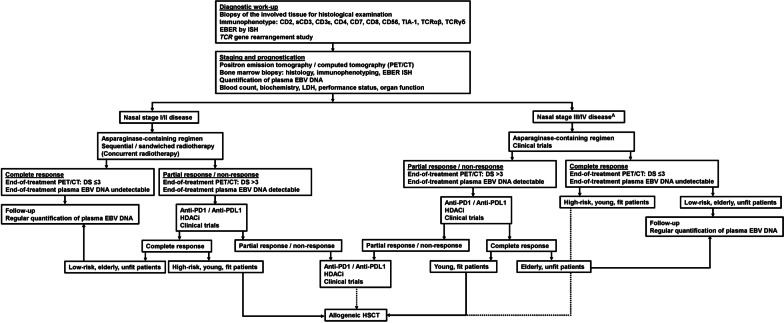
Natural killer (NK)/T-cell lymphomas are aggressive malignancies with a predilection for Asian and South American populations. Epstein-Barr virus (EBV) infection in lymphoma cells is universal. Predominantly extranodal, NK/T-cell lymphomas are divided clinically into nasal (involving the nose and upper aerodigestive tract), non-nasal (involving the skin, gastrointestinal tract, testes, and other organs), and aggressive leukaemia/lymphoma (involving the marrow and multiple organs) subtypes. Initial assessment should include imaging with positron emission tomography computed tomography (PET/CT), quantification of plasma EBV DNA as a surrogate marker of lymphoma load, and bone marrow examination with in situ hybridization for EBV-encoded small RNA. Prognostication can be based on presentation parameters (age, stage, lymph node involvement, clinical subtypes, and EBV DNA), which represent patient factors and lymphoma load; and dynamic parameters during treatment (serial plasma EBV DNA and interim/end-of-treatment PET/CT), which reflect response to therapy. Therapeutic goals are to achieve undetectable plasma EBV DNA and normal PET/CT (Deauville score ≤ 3). NK/T-cell lymphomas express the multidrug resistance phenotype, rendering anthracycline-containing regimens ineffective. Stage I/II nasal cases are treated with non-anthracycline asparaginase-based regimens plus sequential/concurrent radiotherapy. Stage III/IV nasal, and non-nasal and aggressive leukaemia/lymphoma cases are treated with asparaginase-containing regimens and consolidated by allogeneic haematopoietic stem cell transplantation (HSCT) in suitable patients. Autologous HSCT does not improve outcome. In relapsed/refractory cases, novel approaches comprise immune checkpoint blockade of PD1/PD-L1, EBV-specific cytotoxic T-cells, monoclonal antibodies, and histone deacetylase inhibitors. Future strategies may include inhibition of signalling pathways and driver mutations, and immunotherapy targeting the lymphoma and its microenvironment.
自然杀伤(NK)/T 细胞淋巴瘤是一种侵袭性恶性肿瘤,亚洲和南美洲人群中发病率较高。淋巴瘤细胞中普遍存在 Epstein-Barr 病毒(EBV)感染。NK/T 细胞淋巴瘤主要为结外病变,临床上分为鼻型(累及鼻和上呼吸道)、鼻外型(累及皮肤、胃肠道、睾丸和其他器官)和侵袭性白血病/淋巴瘤(累及骨髓和多个器官)亚型。初始评估应包括正电子发射断层扫描计算机断层扫描(PET/CT)成像、血浆 EBV DNA 定量作为淋巴瘤负荷的替代标志物,以及用 EBV 编码的小 RNA 进行原位杂交的骨髓检查。预后可基于表现参数(年龄、分期、淋巴结受累、临床亚型和 EBV DNA),这些参数代表患者因素和淋巴瘤负荷;以及治疗期间的动态参数(连续的血浆 EBV DNA 和治疗期间/结束时的 PET/CT),反映对治疗的反应。治疗目标是实现不可检测的血浆 EBV DNA 和正常的 PET/CT(Deauville 评分≤3)。NK/T 细胞淋巴瘤表达多药耐药表型,使含蒽环类药物的方案无效。I/II 期鼻型病例采用不含蒽环类药物的含 asparaginase 方案联合序贯/同期放疗。III/IV 期鼻型和鼻外型及侵袭性白血病/淋巴瘤病例采用含 asparaginase 的方案治疗,并在合适的患者中通过异基因造血干细胞移植(HSCT)巩固。自体 HSCT 并不能改善预后。在复发/难治性病例中,新的方法包括 PD1/PD-L1 的免疫检查点阻断、EBV 特异性细胞毒性 T 细胞、单克隆抗体和组蛋白去乙酰化酶抑制剂。未来的策略可能包括抑制信号通路和驱动突变,以及针对淋巴瘤及其微环境的免疫治疗。