Hou Mimi M, Barrett Jordan R, Themistocleous Yrene, Rawlinson Thomas A, Diouf Ababacar, Martinez Francisco J, Nielsen Carolyn M, Lias Amelia M, King Lloyd D W, Edwards Nick J, Greenwood Nicola M, Kingham Lucy, Poulton Ian D, Khozoee Baktash, Goh Cyndi, Mac Lochlainn Dylan J, Salkeld Jo, Guilotte-Blisnick Micheline, Huon Christèle, Mohring Franziska, Reimer Jenny M, Chauhan Virander S, Mukherjee Paushali, Biswas Sumi, Taylor Iona J, Lawrie Alison M, Cho Jee-Sun, Nugent Fay L, Long Carole A, Moon Robert W, Miura Kazutoyo, Silk Sarah E, Chitnis Chetan E, Minassian Angela M, Draper Simon J
Department of Biochemistry, University of Oxford, Oxford, OX1 3QU, UK.
The Jenner Institute, University of Oxford, Oxford, OX3 7DQ, UK.
medRxiv. 2022 May 30:2022.05.27.22275375. doi: 10.1101/2022.05.27.22275375.
There are no licensed vaccines against , the most common cause of malaria outside of Africa.
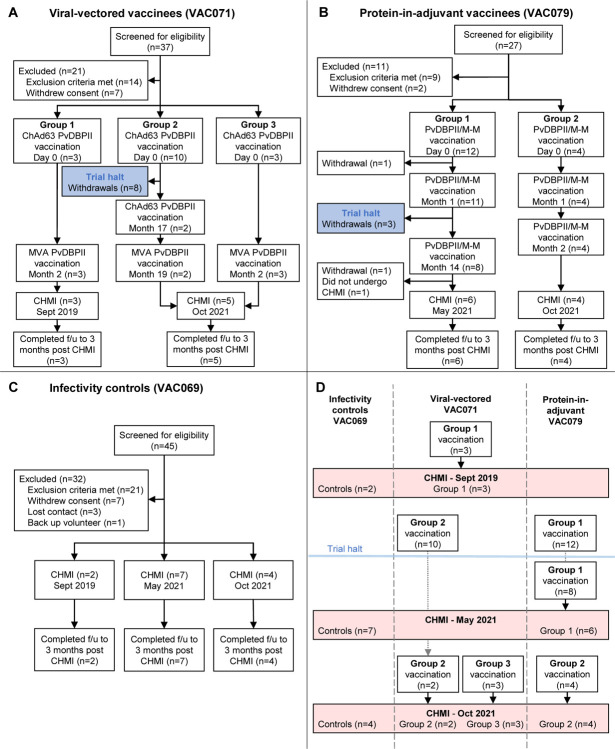
We conducted two Phase I/IIa clinical trials to assess the safety, immunogenicity and efficacy of two vaccines targeting region II of Duffy-binding protein (PvDBPII). Recombinant viral vaccines (using ChAd63 and MVA vectors) were administered at 0, 2 months or in a delayed dosing regimen (0, 17, 19 months), whilst a protein/adjuvant formulation (PvDBPII/Matrix-M™) was administered monthly (0, 1, 2 months) or in a delayed dosing regimen (0, 1, 14 months). Delayed regimens were due to trial halts during the COVID-19 pandemic. Volunteers underwent heterologous controlled human malaria infection (CHMI) with blood-stage parasites at 2-4 weeks following their last vaccination, alongside unvaccinated controls. Efficacy was assessed by comparison of parasite multiplication rate (PMR) in blood post-CHMI, modelled from parasitemia measured by quantitative polymerase-chain-reaction (qPCR).
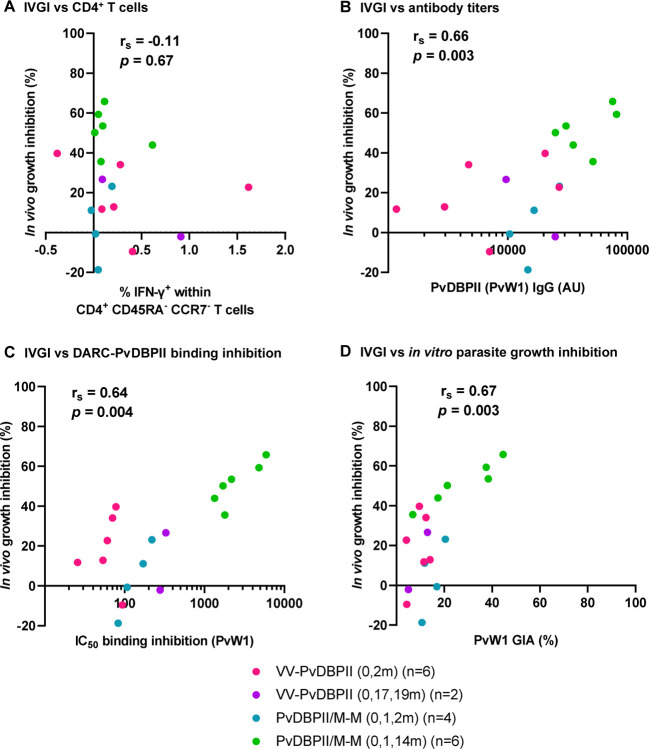
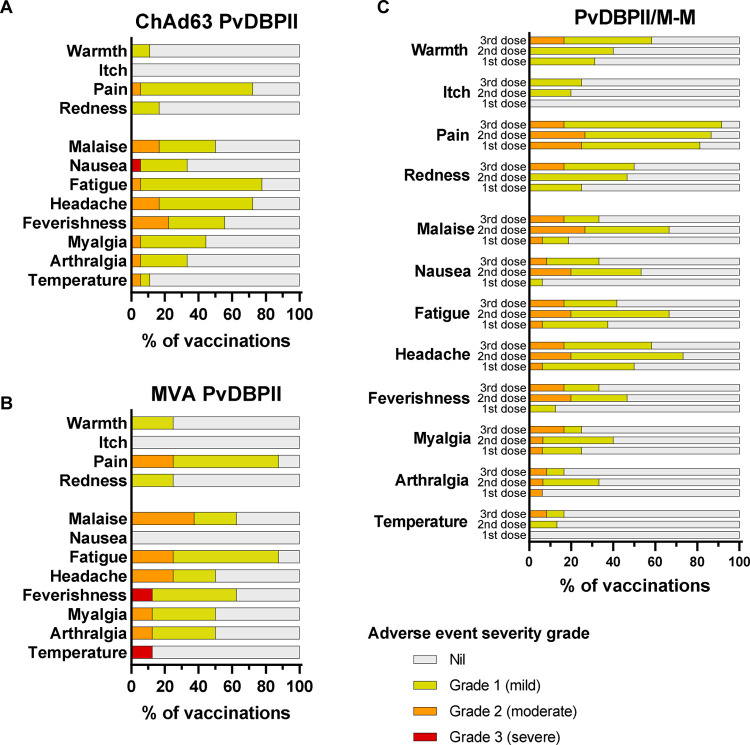
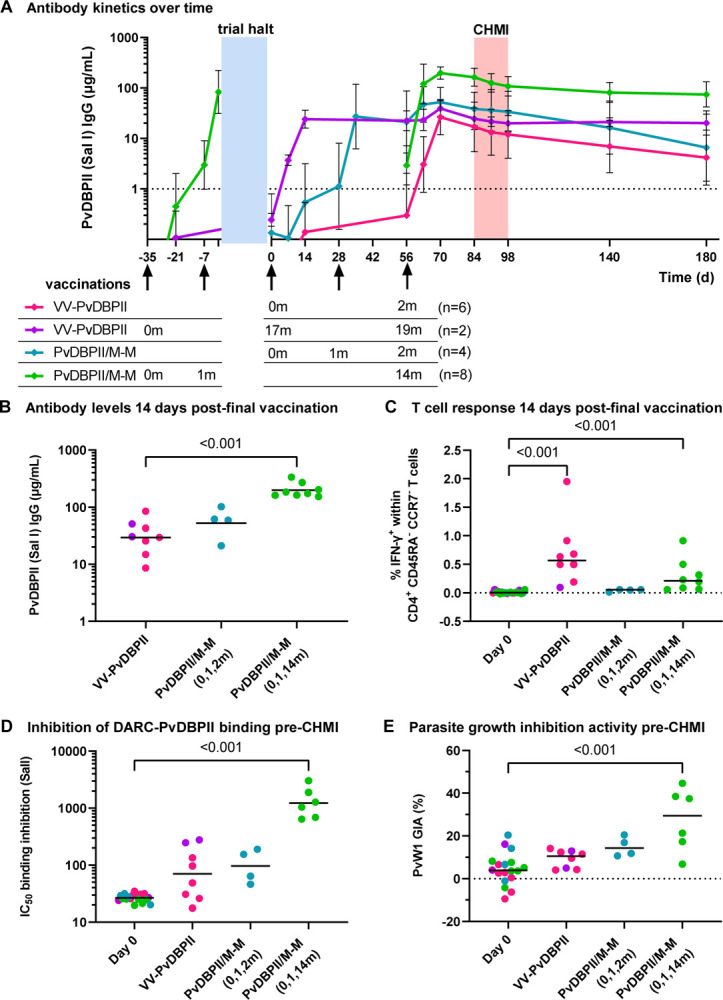
Thirty-two volunteers were enrolled and vaccinated (n=16 for each vaccine). No safety concerns were identified. PvDBPII/Matrix-M™, given in the delayed dosing regimen, elicited the highest antibody responses and reduced the mean PMR following CHMI by 51% (range 36-66%; n=6) compared to unvaccinated controls (n=13). No other vaccine or regimen impacted parasite growth. growth inhibition of blood-stage correlated with functional antibody readouts of vaccine immunogenicity.
Vaccination of malaria-naïve adults with a delayed booster regimen of PvDBPII/ Matrix-M™ significantly reduces the growth of blood-stage . Funded by the European Commission and Wellcome Trust; VAC069, VAC071 and VAC079 ClinicalTrials.gov numbers NCT03797989 , NCT04009096 and NCT04201431 .
对于非洲以外最常见的疟疾病因——[具体疟原虫名称未给出],尚无获批的疫苗。
我们开展了两项I/IIa期临床试验,以评估两种针对达菲结合蛋白(PvDBPII)II区的疫苗的安全性、免疫原性和有效性。重组病毒疫苗(使用ChAd63和MVA载体)在0、2个月时或采用延迟给药方案(0、17、19个月)接种,而蛋白/佐剂制剂(PvDBPII/Matrix-M™)每月(0、1、2个月)或采用延迟给药方案(0、1、14个月)接种。延迟方案是由于在新冠疫情期间试验暂停。志愿者在最后一次接种后2至4周,与未接种的对照者一起接受血液期[具体疟原虫名称未给出]寄生虫的异源控制性人体疟疾感染(CHMI)。通过比较CHMI后血液中寄生虫增殖率(PMR)来评估有效性,PMR由定量聚合酶链反应(qPCR)测量的疟原虫血症建模得出。
32名志愿者入组并接种疫苗(每种疫苗16名)。未发现安全问题。采用延迟给药方案的PvDBPII/Matrix-M™引发了最高的抗体反应,与未接种的对照者(n = 13)相比,CHMI后平均PMR降低了51%(范围36 - 66%;n = 6)。没有其他疫苗或方案影响寄生虫生长。血液期[具体疟原虫名称未给出]的生长抑制与疫苗免疫原性的功能性抗体读数相关。
用PvDBPII/Matrix-M™的延迟加强方案对未感染过疟疾的成年人进行疫苗接种可显著降低血液期[具体疟原虫名称未给出]的生长。由欧盟委员会和惠康信托基金会资助;VAC069、VAC071和VAC079;ClinicalTrials.gov编号NCT03797989、NCT04009096和NCT04201431。