Fondazione IRCCS Policlinico San Matteo.
.
Acta Biomed. 2022 Jun 6;93(S3):e2022145. doi: 10.23750/abm.v93iS3.13067.
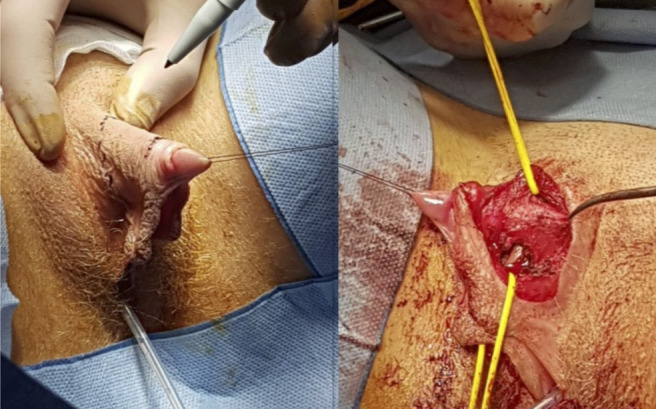
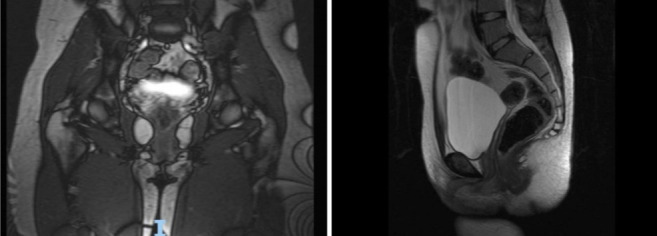
Disorders of sexual differentiation (DSD) with karyotype 46,XY include gonadal developmental differences such as complete gonadal dysgenesis, partial gonadal dysgenesis, testicular regression and ovotesticular sexual differentiation disorder, differences in androgen synthesis or action, such as androgen synthesis deficiency, androgen action deficits, LH receptor deficiency, AMH synthesis or action deficits, and other conditions such as severe hypospadias, cloaca estrophy, etc. Methods: A 17 years-old girl came to our attention for hirsutism, clitoral hypertrophy, primary amenorrhea, and bilateral mammary hypoplasia. According to clinical features and anamnesis, the diagnosis of 46, XY DSD was made. For diagnostic purposes, she underwent an extensive genetic analysis, hormone dosage and instrumental examinations. After a clitoridoplasty and hormone replacement treatment, the patient performs appropriate multidisciplinary follow-up and regular psychotherapy.
The clinical case reported falls, according to the recent classification developed by the Chicago Consensus, within the scope of DSD with karyotype 46, XY. About 160 cases of patients with 17β-HSD3 deficiency, diagnosed at a mean age of 12 years, are described in the literature, most of them coming from Western Asia and Europe and only three cases from Eastern Asia. Clinically, about 30% of patients showed virilization, 20% clitoromegaly, ambiguous genitalia, inguinal/labial mass, 16% primary amenorrhea, and 5% absence of mammary development, features that are partly traced in the case described here.
This case underscores the complexity of managing individuals with DSD. Having acquired the concept that irreversible surgery should be avoided, except in cases where failure to do so would determine health risks, the primary objective of the medical decision lies in meeting conditions aimed at harmonious sexual identification, especially regarding sexual activity and fertility, involving a team of experienced professionals (psychologists, pediatricians, surgeons, endocrinologists, radiologists), capable of promptly identifying suggestive clinical signs.
性发育障碍(DSD)伴核型 46,XY 包括性腺发育差异,如完全性腺发育不全、部分性腺发育不全、睾丸退化和卵睾性性分化障碍,雄激素合成或作用差异,如雄激素合成缺陷、雄激素作用缺陷、LH 受体缺陷、AMH 合成或作用缺陷,以及其他情况,如严重尿道下裂、会阴横隔等。方法:一名 17 岁女孩因多毛症、阴蒂肥大、原发性闭经和双侧乳房发育不全前来就诊。根据临床特征和病史,诊断为 46,XY DSD。为了诊断目的,她接受了广泛的遗传分析、激素剂量和仪器检查。在进行阴蒂整形术和激素替代治疗后,患者进行了适当的多学科随访和定期心理治疗。
报告的临床病例根据最近由芝加哥共识制定的分类,属于核型 46,XY 的 DSD 范围。文献中描述了 17β-HSD3 缺陷症患者约 160 例,平均年龄为 12 岁,他们大多来自西亚和欧洲,只有 3 例来自东亚。临床上,约 30%的患者出现男性化,20%的阴蒂肥大,生殖器模糊,腹股沟/阴唇肿块,16%的原发性闭经,5%的乳房发育缺失,这些特征部分反映了这里描述的病例。
这个病例突出了管理 DSD 患者的复杂性。在获得了除了不进行不可逆手术会导致健康风险之外,应避免进行不可逆手术的概念后,医疗决策的主要目标在于满足旨在促进性认同和谐的条件,特别是在涉及有经验的专业人员(心理学家、儿科医生、外科医生、内分泌学家、放射科医生)的性活动和生育能力方面,能够及时识别出有提示性的临床迹象。