Department of Neurosurgery, Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Skull Base Research Center, Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
BMC Endocr Disord. 2022 Jun 9;22(1):154. doi: 10.1186/s12902-022-01069-5.
Cushing's disease (CD) is among the most common etiologies of hypercortisolism. Magnetic resonance imaging (MRI) is often utilized in the diagnosis of CD, however, up to 64% of adrenocorticotropic hormone (ACTH)-producing pituitary microadenomas are undetectable on MRI. We report 15 cases of MRI negative CD who underwent surgical resection utilizing a purely endoscopic endonasal approach.
Endoscopic endonasal transsphenoidal surgery (EETS) was performed on 134 CD cases by a single surgeon. Fifteen cases met inclusion criteria: no conclusive MRI studies and no previous surgical treatment. Data collected included signs/symptoms, pre- and post-operative hormone levels, and complications resulting from surgical or medical management. Data regarding tumor diameter, location, and tumor residue/recurrence was obtained from both pre- and post-operative MRI. Immunohistochemistry was performed to assess for tumor hormone secretion.
Aside from a statistically significant difference (P = 0.001) in histopathological results between patients with negative and positive MRI, there were no statistically significant difference between these two groups in any other demographic or clinical data point. Inferior petrosal sinus sampling (IPSS) with desmopressin (DDAVP®) administration was performed on the 15 patients with inconclusive MRIs to identify the origin of ACTH hypersecretion via a central/peripheral (C/P) ratio. IPSS in seven, five and three patients showed right, left, and central side lateralization, respectively. With a mean follow-up of 5.5 years, among MRI-negative patients, 14 (93%) and 12 patients (80%) achieved early and long-term remission, respectively. In the MRI-positive cohort, over a mean follow-up of 4.8 years, 113 patients (94.9%) and 102 patients (85.7%) achieved initial and long-term remission, respectively.
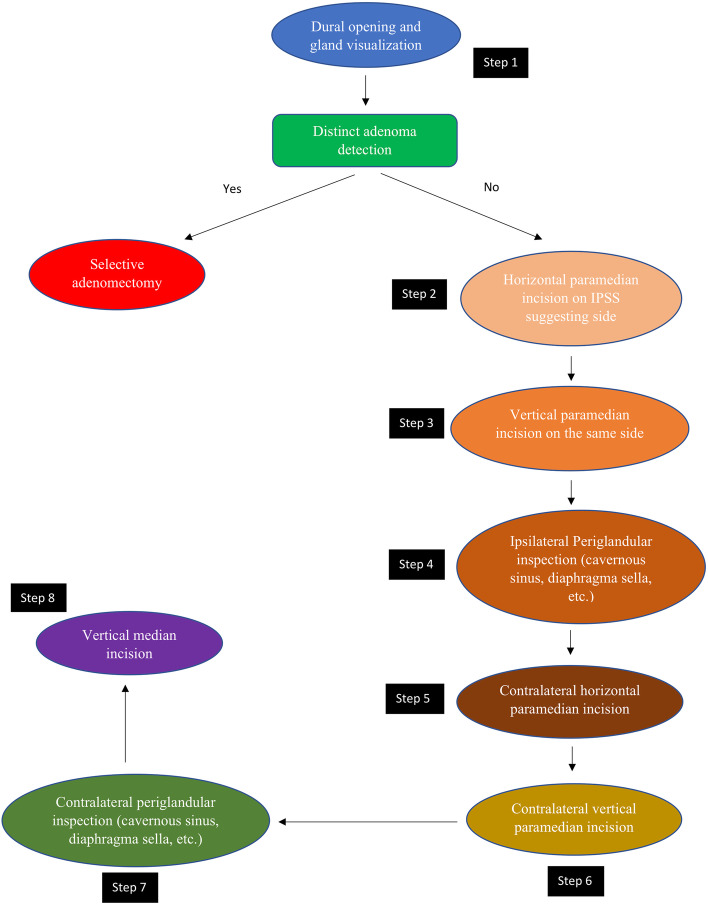
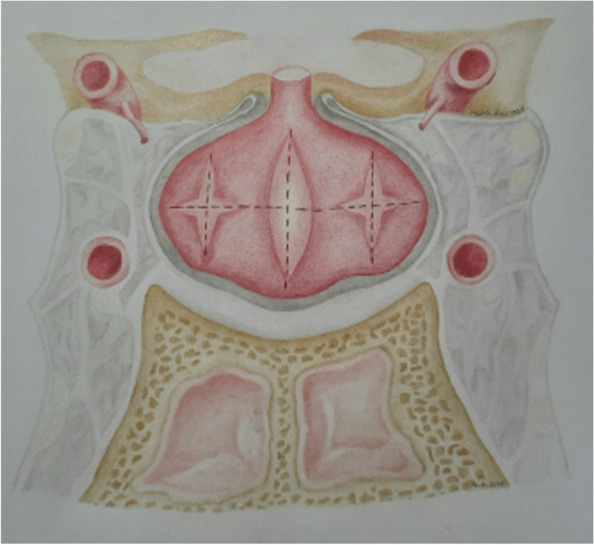
Surgical management of MRI-negative/inconclusive Cushing's disease is challenging scenario requiring a multidisciplinary approach. An experienced neurosurgeon, in collaboration with a dedicated endocrinologist, should identify the most likely location of the adenoma utilizing IPSS findings, followed by careful surgical exploration of the pituitary to identify the adenoma.
库欣病(CD)是最常见的皮质醇增多症病因之一。磁共振成像(MRI)常用于 CD 的诊断,但多达 64%的促肾上腺皮质激素(ACTH)分泌性垂体微腺瘤在 MRI 上无法检测到。我们报告了 15 例 MRI 阴性 CD 患者,他们通过纯内镜经鼻蝶入路接受了手术切除。
一位外科医生对 134 例 CD 患者进行了内镜经鼻蝶窦手术(EETS)。15 例符合纳入标准:无明确 MRI 研究和无先前手术治疗。收集的数据包括体征/症状、术前和术后激素水平以及手术或药物治疗引起的并发症。从术前和术后 MRI 中获得肿瘤直径、位置和肿瘤残留/复发的数据。进行免疫组织化学检查以评估肿瘤激素分泌。
除了 MRI 阴性和阳性患者的组织病理学结果有统计学显著差异(P=0.001)外,两组间在任何其他人口统计学或临床数据点均无统计学显著差异。对 15 例 MRI 结果不确定的患者进行了蝶鞍旁窦取样(IPSS)联合去氨加压素(DDAVP®)给药,通过中央/周围(C/P)比值来确定 ACTH 分泌过度的起源。IPSS 结果分别显示右侧、左侧和中央侧偏位的患者各有 7 例、5 例和 3 例。在 5.5 年的平均随访中,MRI 阴性患者中,14 例(93%)和 12 例(80%)分别在早期和长期缓解,MRI 阳性患者中,在 4.8 年的平均随访中,113 例(94.9%)和 102 例(85.7%)分别在初始和长期缓解。
MRI 阴性/不确定的库欣病的手术治疗是一个具有挑战性的情况,需要多学科方法。有经验的神经外科医生应与专门的内分泌学家合作,利用 IPSS 结果确定腺瘤最有可能的位置,然后仔细探查垂体以识别腺瘤。