Medicus Economics, LLC, 2 Stonehill Lane, Milton, MA, 02186, USA.
Kite, A Gilead Company, 2400 Broadway, Santa Monica, CA, 90404, USA.
Adv Ther. 2022 Aug;39(8):3560-3577. doi: 10.1007/s12325-022-02188-0. Epub 2022 Jun 11.
Cost-effectiveness data on chimeric antigen receptor (CAR) T cell therapies for relapsed/refractory large B cell lymphoma (R/R LBCL), accounting for inpatient/outpatient site of care (site), are sparse.
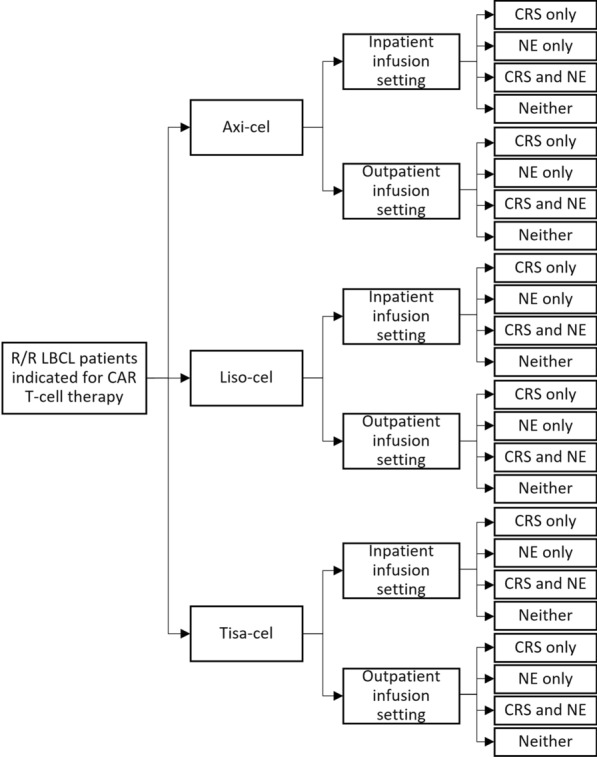
This payer model compares lifetime costs/benefits for CAR T cell-treated (axicabtagene ciloleucel [axi-cel], lisocabtagene maraleucel [liso-cel], tisagenlecleucel [tisa-cel]) patients with R/R LBCL in the USA. Three-month post-infusion costs were derived from unit costs and real-world all-payer (RW) site-specific utilization data for 1175 patients with diffuse R/R LBCL (CAR T cell therapy October 2017-September 2020). Therapy- and site-specific grade 3+ cytokine release syndrome (CRS) and neurologic event (NE) incidences were imputed from published trials. Lifetime quality-adjusted life-years (QALYs) and long-term costs were calculated from therapy-specific overall and progression-free survival data, adjusted for differences in trial populations. The base case used 17% outpatient site (RW) for all therapies. ZUMA-1 trial cohorts 1/2 informed other axi-cel base case inputs; ZUMA-1 cohorts 4/6 data (updated safety management) supported scenario analyses.
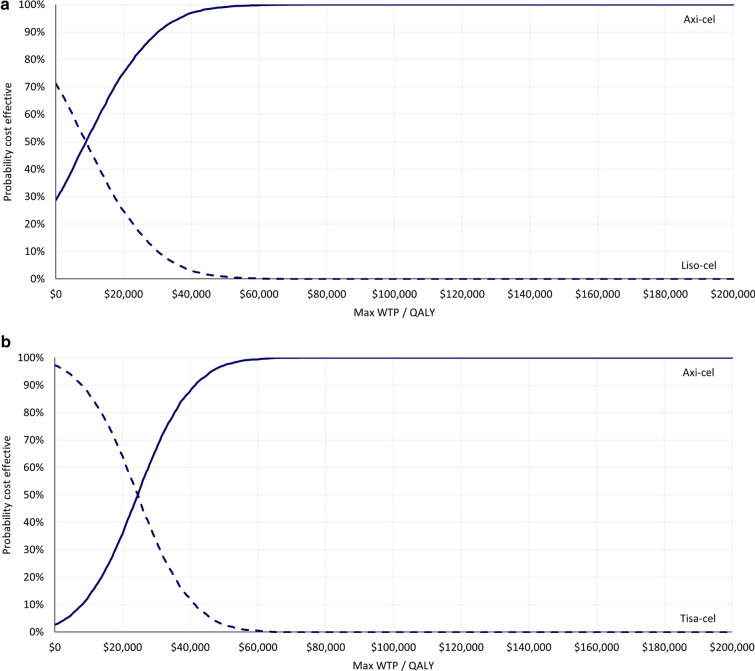
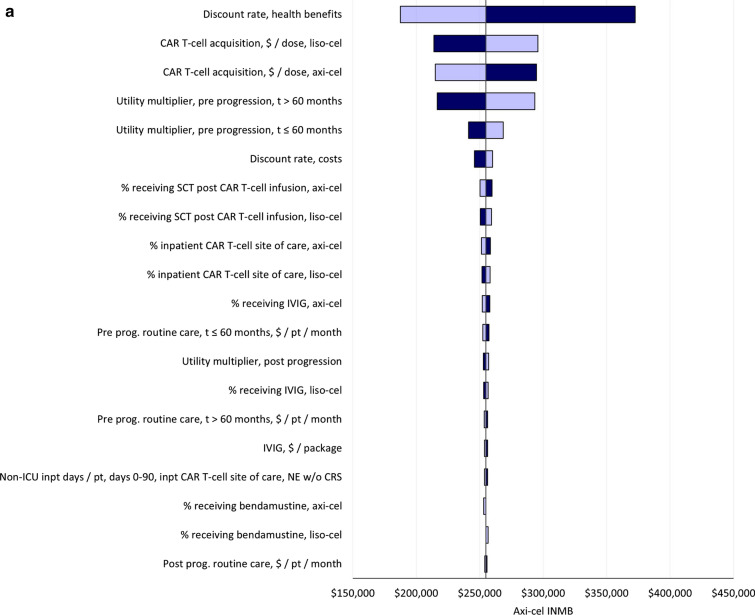
Base case total costs for axi-cel exceeded liso-cel ($637 K versus $621 K) and tisa-cel ($631 K versus $577 K) costs. Three-month post-infusion costs were $57 K to $59 K across all therapies. Total QALYs for axi-cel also exceeded those for liso-cel (7.7 versus 5.9) and tisa-cel (7.2 versus 5.0) with incremental costs per QALY gained of $9 K versus liso-cel and $25 K versus tisa-cel. Base case incremental net monetary benefit was $255 K (95% confidence interval (CI) $181-326 K) for axi-cel versus liso-cel, and $280 K (95% CI $200-353 K) versus tisa-cel. Longer survival with axi-cel conferred higher lifetime costs. In all scenarios (e.g., varied outpatient proportions, CRS/NE incidence), axi-cel was cost-effective versus both comparators at a maximum willingness-to-pay of under $26 K/QALY as a result of axi-cel's higher incremental survival gains and quality-of-life.
Axi-cel is a cost-effective CAR T cell therapy for patients with R/R LBCL compared to tisa-cel and liso-cel. Site of care does not impact the cost-effectiveness of CAR T cell therapy.
针对复发/难治性大 B 细胞淋巴瘤(R/R LBCL)患者,嵌合抗原受体(CAR)T 细胞疗法的成本效益数据,考虑到住院/门诊治疗地点(地点),十分匮乏。
本项支付者模型比较了在美国接受 CAR T 细胞治疗(axicabtagene ciloleucel [axi-cel]、lisocabtagene maraleucel [liso-cel]、tisagenlecleucel [tisa-cel])的 R/R LBCL 患者的终生成本/效益。从 1175 名弥漫性 R/R LBCL 患者(2017 年 10 月至 2020 年 9 月接受 CAR T 细胞治疗)的单位成本和真实世界全支付者(RW)特定地点利用数据中得出了输注后三个月的成本。根据已发表的试验,对治疗和特定部位的 3+级细胞因子释放综合征(CRS)和神经事件(NE)发生率进行了推断。根据特定疗法的总体生存率和无进展生存率数据,计算了终生质量调整生命年(QALY)和长期成本,并根据试验人群的差异进行了调整。基础情况使用了所有疗法 17%的门诊治疗地点(RW)。ZUMA-1 试验队列 1/2 为 axi-cel 的基础情况输入提供了信息;ZUMA-1 队列 4/6 的数据(更新了安全管理)支持了方案分析。
axi-cel 的总治疗成本高于 liso-cel(637 万美元对 621 万美元)和 tisa-cel(631 万美元对 577 万美元)。所有疗法的输注后三个月成本均为 57000 美元至 59000 美元。axi-cel 的总 QALY 也高于 liso-cel(7.7 对 5.9)和 tisa-cel(7.2 对 5.0),增量每获得一个 QALY 的成本分别为 9000 美元对 liso-cel 和 25000 美元对 tisa-cel。axi-cel 相对于 liso-cel 的基础情况增量净货币收益为 255 万美元(95%置信区间(CI)为 181-326 万美元),相对于 tisa-cel 为 280 万美元(95% CI 为 200-353 万美元)。axi-cel 的生存时间更长,导致终生成本更高。在所有情况下(例如,门诊比例不同、CRS/NE 发生率),由于 axi-cel 的增量生存获益和生活质量更高,axi-cel 相较于两种对照药物,在最高支付意愿低于 26000 美元/QALY 的情况下,均具有成本效益。
与 tisa-cel 和 liso-cel 相比,axi-cel 是一种用于治疗 R/R LBCL 患者的具有成本效益的 CAR T 细胞疗法。治疗地点不会影响 CAR T 细胞疗法的成本效益。