Utsumi Akari, Goto Yuri, Suzuki Takaaki, Imai Chiaki, Matsui Shinichiro, Sakaida Emiko, Ishii Itsuko
Division of Pharmacy, Chiba University Hospital, 1-8-1 Inohana Chuo-ku, Chiba, 260-8677, Japan.
Division of Hematology, Department of Clinical Cell Biology, Chiba University Graduate School of Medicine, Chiba, Japan.
J Pharm Health Care Sci. 2022 Jun 11;8(1):17. doi: 10.1186/s40780-022-00247-w.
Nelarabine is an antineoplastic purine analog used for the treatment of refractory or relapsed T-cell acute lymphoblastic leukemia (T-ALL). The most prominent side effect of nelarabine are neurotoxicity and hematologic disorder, which are considered dose-limiting factors. Although clinical studies have reported myopathy due to nelarabine, actual detailed outcomes were not well-known initial approval. The incidence of nelarabine induced rhabdomyolysis has been reported at 2% in study in children. Cases of rhabdomyolysis have been reported in adults from medical facilities in the United Sates with renal dysfunction or severe muscle symptoms after administration of multiple courses of nelarabine. In this report, we discuss a case of rhabdomyolysis diagnosed after a single course of nelarabine. In this case, creatine kinase (CK) level was elevated in grade 4, without renal dysfunction and severe muscle symptoms.
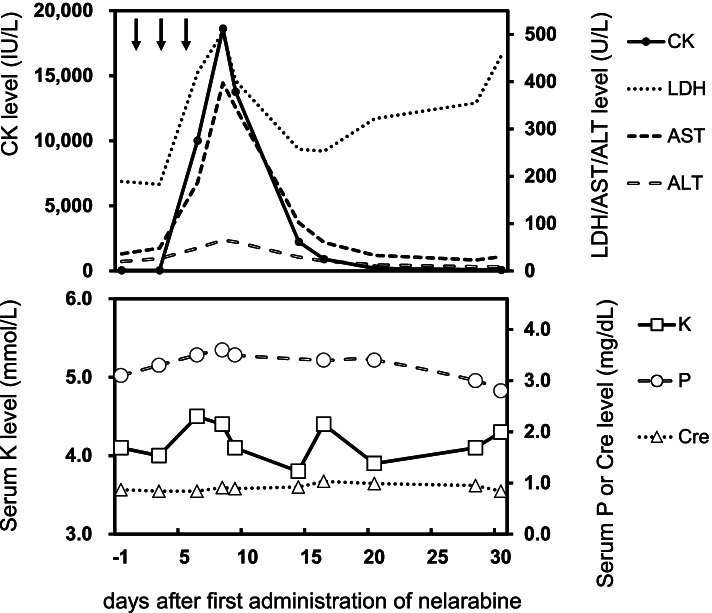
A 46-year-old man from Japan was diagnosed with T-ALL and received a hematopoietic stem cell transplantation in first remission. However, the disease relapsed 6 months after transplantation. Nelarabine was selected as the next-line chemotherapeutic agent. The patient received 1500 mg/m of nelarabine on day 1 followed by a dose on days 3 and 5. CK levels, which were baseline before treatment, increased to grade 4 (18,620 IU/L) on the 8th day of treatment. He was diagnosed as rhabdomyolysis due to nelarabine with little possibility of other factors. He complained only of mild pain in his upper extremities and no other symptoms were noticed. The patient was managed with hydration. The pain lasted approximately 7 days, but there were no sequelae secondary to the rhabdomyolysis. Because of the elevation of CK in grade 4, we avoided re-administration.
In the patient administrated nelarabine, CK level was elevated in grade 4, without other symptoms of rhabdomyolysis. The results suggest that CK may be elevated at the onset of rhabdomyolysis caused by nelarabine, even in the absence of other symptoms. Therefore, it was suggested that monitoring CK during nelarabine administration is important for detecting rhabdomyolysis before it becomes severe. We consider that CK should be monitored even in absence of symptoms.
奈拉滨是一种抗肿瘤嘌呤类似物,用于治疗难治性或复发性T细胞急性淋巴细胞白血病(T-ALL)。奈拉滨最突出的副作用是神经毒性和血液系统紊乱,这些被认为是剂量限制因素。尽管临床研究报告了奈拉滨引起的肌病,但在最初获批时实际的详细结果并不为人所知。在儿童研究中,奈拉滨诱导横纹肌溶解的发生率报告为2%。在美国,有医疗机构报告了成人在接受多个疗程奈拉滨治疗后出现肾功能不全或严重肌肉症状的横纹肌溶解病例。在本报告中,我们讨论了一例在接受单疗程奈拉滨治疗后被诊断为横纹肌溶解的病例。在该病例中,肌酸激酶(CK)水平升高至4级,无肾功能不全和严重肌肉症状。
一名46岁的日本男性被诊断为T-ALL,并在首次缓解期接受了造血干细胞移植。然而,移植后6个月疾病复发。奈拉滨被选为二线化疗药物。患者在第1天接受了1500mg/m²的奈拉滨治疗,随后在第3天和第5天各接受一次剂量。治疗前基线水平的CK水平在治疗第8天升至4级(18,620IU/L)。他被诊断为奈拉滨引起的横纹肌溶解,其他因素导致的可能性很小。他仅抱怨上肢轻度疼痛,未发现其他症状。患者接受了补液治疗。疼痛持续了约7天,但横纹肌溶解未留下后遗症。由于CK升高至4级,我们避免了再次给药。
在接受奈拉滨治疗的患者中,CK水平升高至4级,无横纹肌溶解的其他症状。结果表明,即使在没有其他症状的情况下,奈拉滨引起的横纹肌溶解发作时CK也可能升高。因此,建议在奈拉滨给药期间监测CK对于在横纹肌溶解变得严重之前进行检测很重要。我们认为即使没有症状也应监测CK。