Medical University of Vienna, Center for Pathophysiology, Infectiology and Immunology, Institute of Immunology, Vienna, Austria.
Medical University of Vienna, Center for Pathophysiology, Infectiology and Immunology, Department of Pathophysiology and Allergy Research, Vienna, Austria.
Allergy. 2022 Nov;77(11):3408-3425. doi: 10.1111/all.15406. Epub 2022 Jul 19.
Antibody-based tests are available for measuring SARS-CoV-2-specific immune responses but fast T-cell assays remain scarce. Robust T cell-based tests are needed to differentiate specific cellular immune responses after infection from those after vaccination.
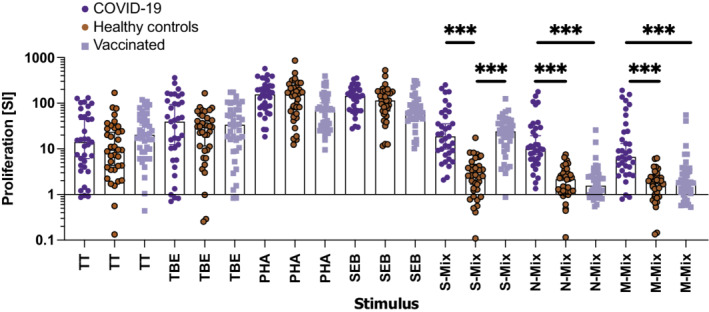
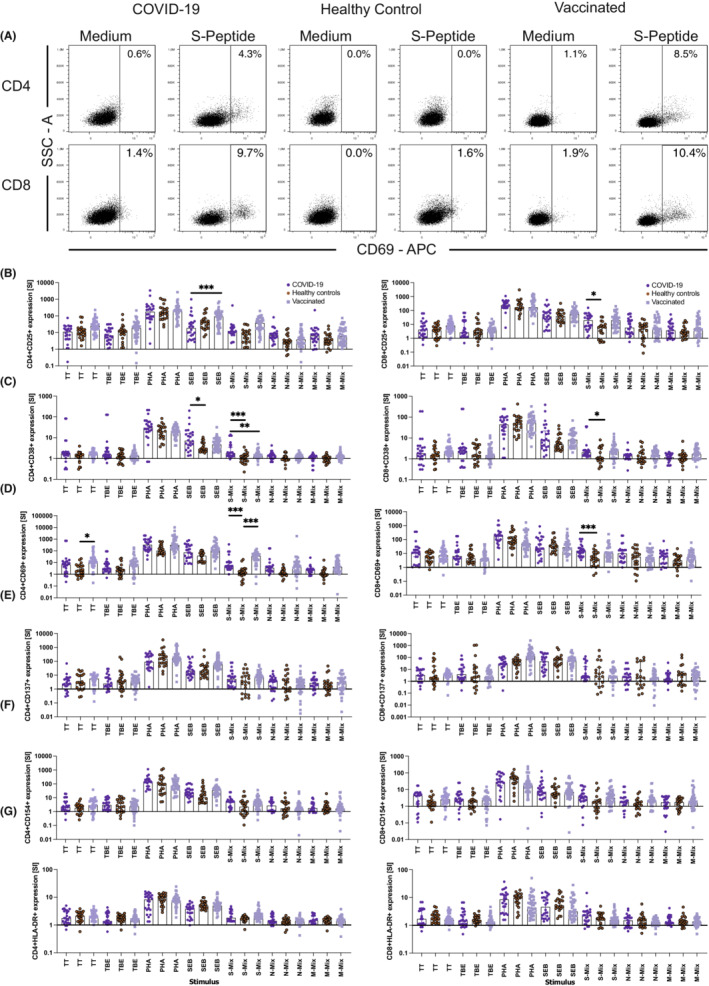
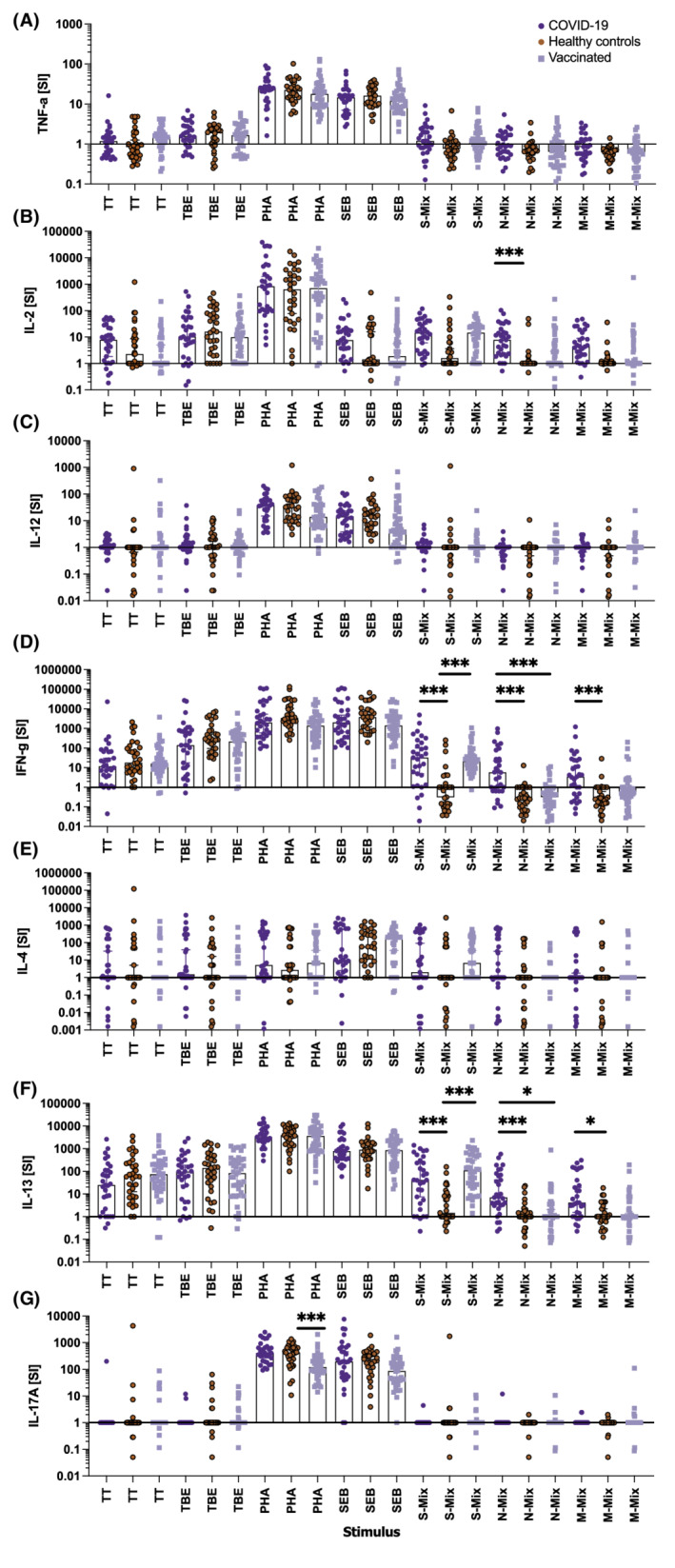
One hundred seventeen individuals (COVID-19 convalescent patients: n = 40; SARS-CoV-2 vaccinees: n = 41; healthy controls: n = 36) were evaluated for SARS-CoV-2-specific cellular immune responses (proliferation, Th1, Th2, Th17, and inflammatory cytokines, activation-induced marker [AIM] expression) by incubating purified peripheral blood mononuclear cells (PBMC) or whole blood (WB) with SARS-CoV-2 peptides (S, N, or M), vaccine antigens (tetanus toxoid, tick borne encephalitis virus) or polyclonal stimuli (Staphylococcal enterotoxin, phytohemagglutinin).
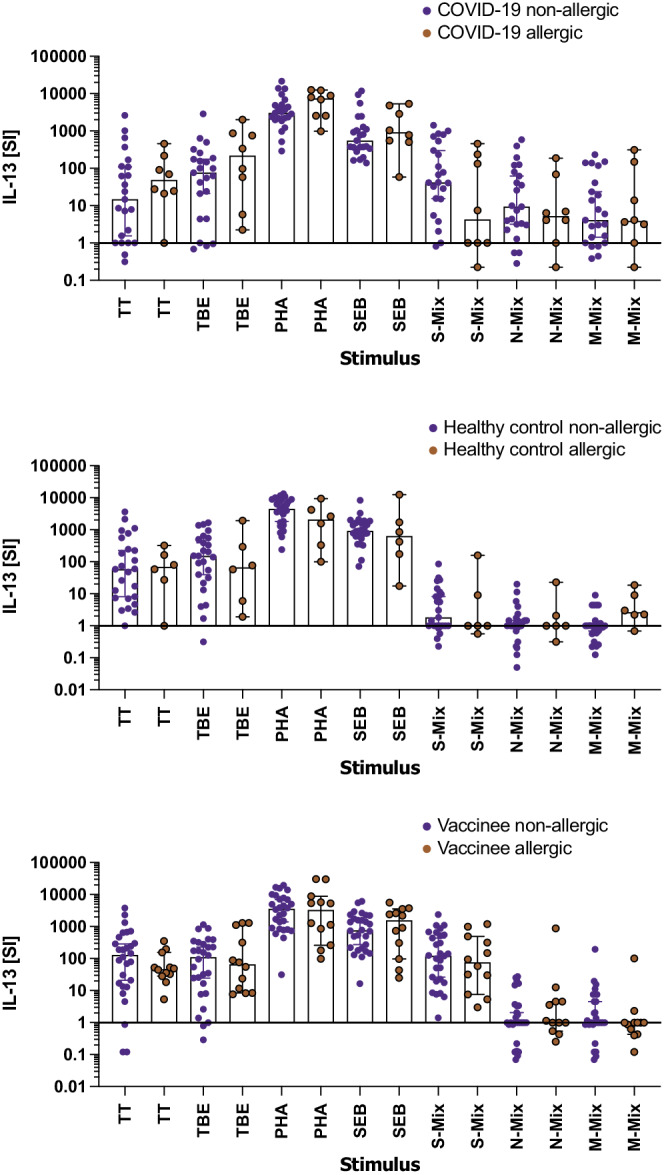
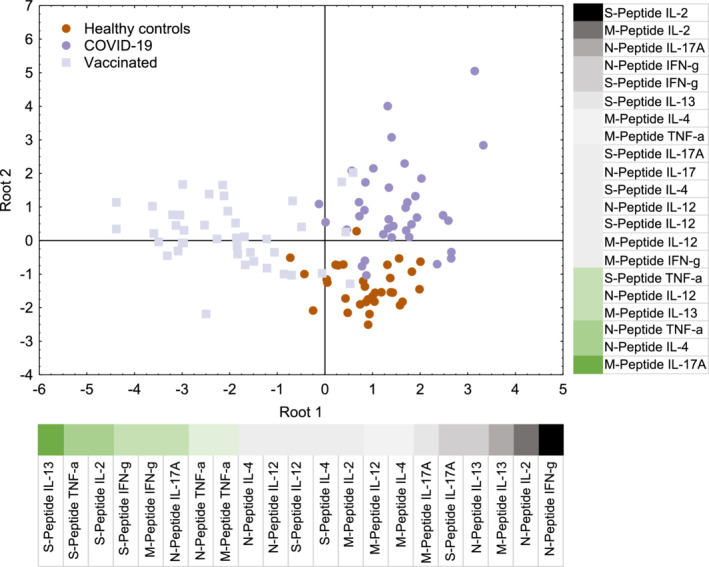
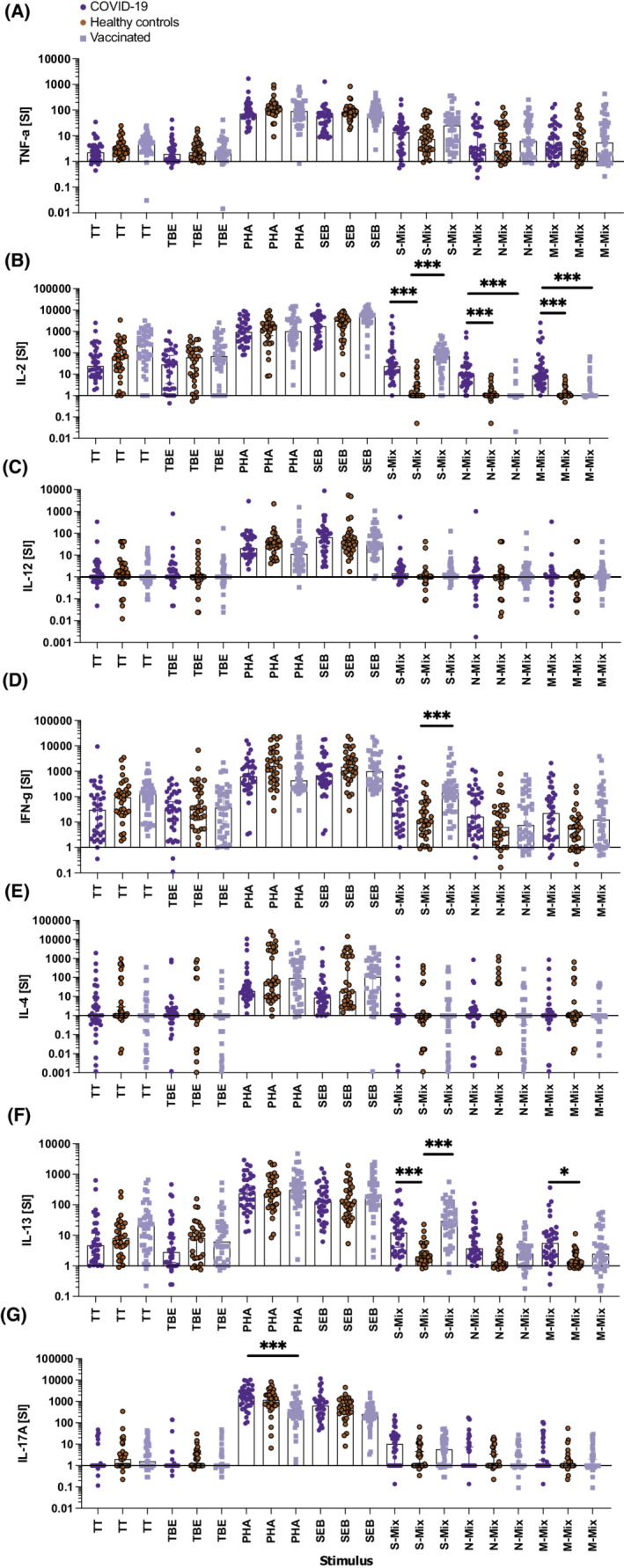
N-peptide mix stimulation of WB identified the combination of IL-2 and IL-13 secretion as superior to IFN-γ secretion to discriminate between COVID-19-convalescent patients and healthy controls (p < .0001). Comparable results were obtained with M- or S-peptides, the latter almost comparably recalled IL-2, IFN-γ, and IL-13 responses in WB of vaccinees. Analysis 10 months as opposed to 10 weeks after COVID-19, but not allergic disease status, positively correlated with IL-13 recall responses. WB cytokine responses correlated with cytokine and proliferation responses of PBMC. Antigen-induced neo-expression of the C-type lectin CD69 on CD4 (p < .0001) and CD8 (p = .0002) T cells informed best about the SARS-CoV-2 exposure status with additional benefit coming from CD25 upregulation.
Along with N- and S-peptide-induced IL-2 and CD69 neo-expression, we suggest to include the type 2 cytokine IL-13 as T-cellular recall marker for SARS-CoV-2 specific T-cellular immune responses after infection and vaccination.
目前已有用于检测 SARS-CoV-2 特异性免疫反应的抗体检测方法,但快速 T 细胞检测方法仍然稀缺。需要稳健的 T 细胞检测方法来区分感染后的特异性细胞免疫反应和接种疫苗后的免疫反应。
评估了 117 名个体(COVID-19 恢复期患者:n=40;SARS-CoV-2 疫苗接种者:n=41;健康对照者:n=36)的 SARS-CoV-2 特异性细胞免疫反应(增殖、Th1、Th2、Th17 和炎症细胞因子、激活诱导标志物[AIM]表达),方法是将纯化的外周血单核细胞(PBMC)或全血(WB)与 SARS-CoV-2 肽(S、N 或 M)、疫苗抗原(破伤风类毒素、蜱传脑炎病毒)或多克隆刺激物(葡萄球菌肠毒素、植物血凝素)孵育。
WB 中 N 肽混合物刺激鉴定出 IL-2 和 IL-13 分泌的组合优于 IFN-γ 分泌,可区分 COVID-19 恢复期患者和健康对照者(p<0.0001)。使用 M 或 S 肽可获得类似的结果,后者在疫苗接种者的 WB 中几乎可相当程度地召回 IL-2、IFN-γ 和 IL-13 反应。与 COVID-19 后 10 周相比,10 个月后(而非过敏疾病状态)与 IL-13 回忆反应呈正相关。WB 细胞因子反应与 PBMC 的细胞因子和增殖反应相关。抗原诱导的 CD4(p<0.0001)和 CD8(p=0.0002)T 细胞上 C 型凝集素 CD69 的新型表达能最好地反映 SARS-CoV-2 的暴露状态,CD25 的上调也有额外益处。
除了 N 和 S 肽诱导的 IL-2 和 CD69 新型表达外,我们还建议将 2 型细胞因子 IL-13 作为感染和接种疫苗后 SARS-CoV-2 特异性 T 细胞免疫反应的 T 细胞回忆标志物。