Department of Gastroenterology, Infectious Diseases and Rheumatology, Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität and Humboldt Universität zu Berlin, Campus Benjamin Franklin, Berlin, Germany.
Deutsches Rheumaforschungszentrum Berlin (DRFZ), An Institute of the Leibniz Association, Berlin, Germany.
BMC Infect Dis. 2022 Jun 13;22(1):537. doi: 10.1186/s12879-022-07513-0.
Passive immunization against SARS-CoV-2 limits viral burden and death from COVID-19; however, it poses a theoretical risk of disease exacerbation through antibody-dependent enhancement (ADE). ADE after anti-SARS-CoV2 antibody treatment has not been reported, and therefore the potential risk and promoting factors remain unknown.
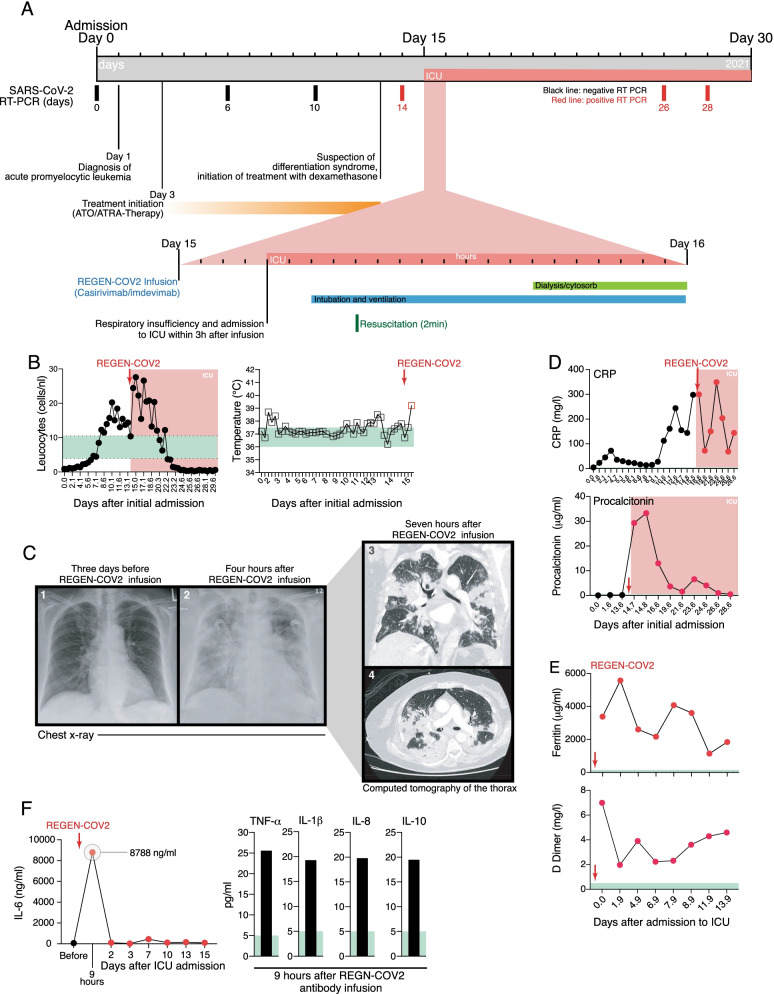
A 75-year-old female was admitted to the emergency room with recurrent, unexplained bruises and leukocytopenia, anemia, and thrombocytopenia. Evaluation of a bone marrow biopsy established the diagnosis of an acute promyelocytic leukemia (APL). SARS-CoV-2 RT-PCR testing of nasal and throat swabs on admission was negative. During the routine SARS-CoV-2 testing of inpatients, our patient tested positive for SARS-CoV-2 on day 14 after admission without typical COVID-19 symptoms. Due to disease- and therapy-related immunosuppression and advanced age conferring a high risk of progressing to severe COVID-19, casirivimab and imdevimab were administered as a preemptive approach. The patient developed immune activation and cytokine release syndrome (CRS) occurring within four hours of preemptive anti-SARS-CoV2 antibody (casirivimab/imdevimab) infusion. Immune activation and CRS were evidenced by a rapid increase in serum cytokines (IL-6, TNFα, IL-8, IL-10), acute respiratory insufficiency, and progressive acute respiratory distress syndrome.
The temporal relationship between therapeutic antibody administration and the rapid laboratory, radiological, and clinical deterioration suggests that CRS was an antibody-related adverse event, potentially exacerbated by APL treatment-mediated differentiation of leukemic blasts and promyelocytes. This case highlights the need for careful assessment of life-threatening adverse events after passive SARS-CoV-2 immunization, especially in the clinical context of patients with complex immune and hematological landscapes.
针对 SARS-CoV-2 的被动免疫可降低 COVID-19 患者的病毒载量和死亡率;然而,它通过抗体依赖性增强(ADE)理论上存在加重疾病的风险。尚未报道抗 SARS-CoV2 抗体治疗后的 ADE,因此潜在风险和促进因素尚不清楚。
一名 75 岁女性因反复出现不明原因瘀斑和白细胞减少症、贫血和血小板减少症而被收入急诊室。骨髓活检评估确立了急性早幼粒细胞白血病(APL)的诊断。入院时鼻和咽喉拭子的 SARS-CoV-2 RT-PCR 检测结果为阴性。在对住院患者进行常规 SARS-CoV-2 检测期间,我们的患者在入院后第 14 天检测出 SARS-CoV-2 呈阳性,且无典型 COVID-19 症状。由于疾病和治疗相关的免疫抑制以及高龄导致发生严重 COVID-19 的风险较高,因此作为预防措施给予 casirivimab 和 imdevimab。患者在预先给予抗 SARS-CoV2 抗体(casirivimab/imdevimab)后 4 小时内发生免疫激活和细胞因子释放综合征(CRS)。免疫激活和 CRS 的证据是血清细胞因子(IL-6、TNFα、IL-8、IL-10)迅速增加、急性呼吸功能不全和进行性急性呼吸窘迫综合征。
治疗性抗体给药与实验室、影像学和临床迅速恶化之间的时间关系表明 CRS 是一种抗体相关的不良事件,可能因 APL 治疗介导的白血病细胞和早幼粒细胞分化而加重。该病例强调了在被动 SARS-CoV-2 免疫接种后需要仔细评估危及生命的不良事件,尤其是在具有复杂免疫和血液学背景的患者的临床环境中。