Jan Muhammad Y, Moe Sharon M, Adebiyi Oluwafisayo, Chen Jeannie, Powelson John, Burney Heather N, Yaqub Muhammad S, Mishler Dennis P, Moorthi Ranjani N, Taber Tim E, Anderson Melissa D, Li Yang, Li Xiaochun, Fridell Jonathan A, Goggins William C, Sharfuddin Asif A
Division of Nephrology and Hypertension, Indiana University School of Medicine, Indianapolis, Indiana, USA.
Indiana Clinical and Translational Sciences Institute, Indianapolis, Indiana, USA.
Kidney Int Rep. 2022 Apr 7;7(6):1364-1376. doi: 10.1016/j.ekir.2022.03.035. eCollection 2022 Jun.
Hypotension after deceased donor kidney transplant (DDKT) is a risk factor for delayed graft function (DGF) and poor graft survival (GS). We hypothesize that vasopressin use in hypotensive DDKT recipients (DDKTRs) to increase blood pressure (BP) reduces DGF rates and is safe without increasing mortality.
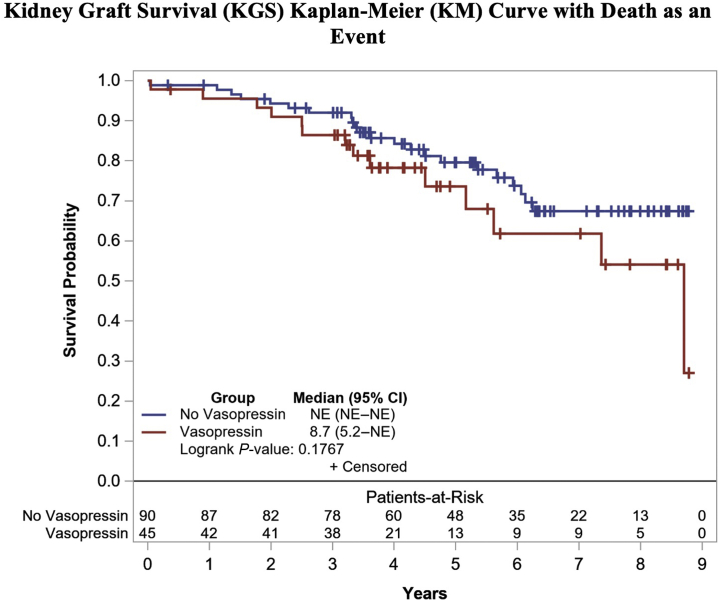
Group with vasopressin "study group" ( 45) was defined as DDKTRs between 2012 and 2017 who required vasopressin for hypotension systolic BP (SBP) <120 mm Hg or diastolic BP (DBP) <60 mm Hg. DDKTRs with no-vasopressin "comparison group" ( 90) were propensity score-matched DDKTRs between 2012 and 2017 without vasopressin use. Primary outcomes were GS, creatinine and allograft biopsy rate at 1 year, DGF rate, and death during transplant hospitalization.
Vasopressin group had lower mean maximum and minimum SBP and DBP in the operating room (OR). Median vasopressin start time post-DDKT was 2 hours (interquartile range [IQR] 1-6), and duration of use was 42 hours (IQR 24-63). DGF, creatinine at 1 year, and allograft biopsy rates were comparable. No deaths occurred during transplant hospitalization. Multivariable analysis did not find an effect of vasopressin use on GS.
Treatment of hypotensive DDKTRs with vasopressin is safe and facilitated similar graft function and survival with that of nonhypotensive patients. In the absence of a randomized control trial, our study supports the safety of vasopressin therapy to prevent the adverse effects of hypotension.
deceased供体肾移植(DDKT)后低血压是移植肾功能延迟恢复(DGF)和移植肾存活率(GS)低的危险因素。我们假设,在低血压的DDKT受者(DDKTRs)中使用血管加压素升高血压可降低DGF发生率,且安全不增加死亡率。
血管加压素组“研究组”(45例)定义为2012年至2017年间因收缩压(SBP)<120mmHg或舒张压(DBP)<60mmHg低血压而需要血管加压素的DDKTRs。无血管加压素组“对照组”(90例)为2012年至2017年间未使用血管加压素且倾向评分匹配的DDKTRs。主要结局指标为1年时的GS、肌酐和移植肾活检率、DGF发生率以及移植住院期间的死亡率。
血管加压素组在手术室(OR)的平均最高和最低SBP及DBP较低。DDKT后血管加压素开始使用的中位时间为2小时(四分位数间距[IQR]1 - 6),使用持续时间为42小时(IQR 24 - 63)。DGF、1年时的肌酐和移植肾活检率相当。移植住院期间无死亡发生。多变量分析未发现使用血管加压素对GS有影响。
用血管加压素治疗低血压的DDKTRs是安全的,移植肾功能和存活率与非低血压患者相似。在缺乏随机对照试验的情况下,我们的研究支持血管加压素治疗预防低血压不良反应的安全性。