National and Kapodistrian University of Athens, Athens, Greece; Frontier Science Foundation Hellas, Athens, Greece.
National University Cancer Institute, Department of Haematology-Oncology, Singapore.
ESMO Open. 2022 Jun;7(3):100507. doi: 10.1016/j.esmoop.2022.100507. Epub 2022 Jun 10.
The ETOP 10-16 BOOSTER trial failed to demonstrate a progression-free survival (PFS) benefit for adding bevacizumab to osimertinib in second line. An exploratory subgroup analysis, however, suggested a PFS benefit of the combination in patients with a smoking history and prompted us to do this study.
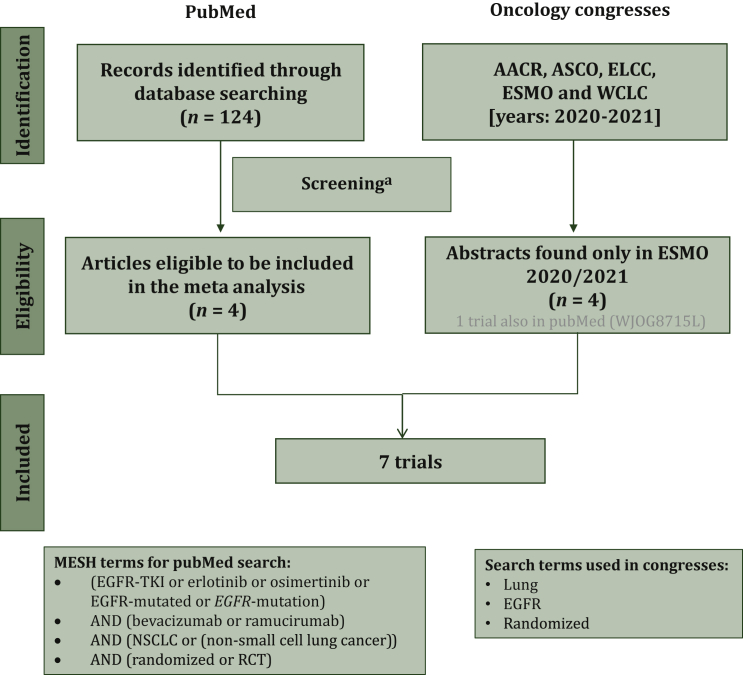
A systematic review and meta-analysis to evaluate the differential effect of smoking status on the benefit of adding an angiogenesis inhibitor to epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitor therapy was carried out. All relevant randomized controlled trials appearing in main oncology congresses or in PubMed as of 1 November 2021 were used according to the Preferred Reporting Items for Systematic Review and Meta-Analyses statement. Primarily PFS according to smoking status, and secondarily overall survival (OS) were of interest. Pooled and interaction hazard ratios (HRs) were estimated by fixed or random effects models, depending on the detected degree of heterogeneity. Bias was assessed using the revised Cochrane tool for randomized controlled trials (RoB 2).
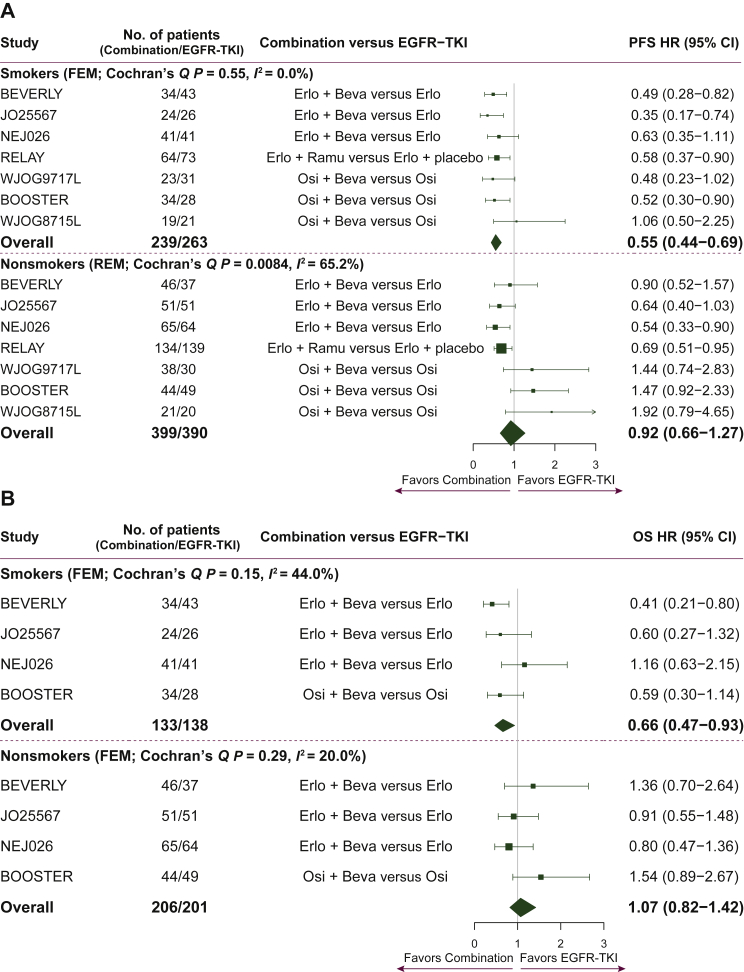
Information by smoking was available for 1291 patients for PFS (seven studies) and 678 patients for OS (four studies). The risk of bias was low for all studies. Combination treatment significantly prolonged PFS for smokers [n = 502, HR = 0.55, 95% confidence interval (CI): 0.44-0.69] but not for nonsmokers (n = 789, HR = 0.92, 95% CI: 0.66-1.27; treatment-by-smoking interaction P = 0.02). Similarly, a significant OS benefit was found for smokers (n = 271, HR = 0.66, 95% CI: 0.47-0.93) but not for nonsmokers (n = 407, HR = 1.07, 95% CI: 0.82-1.42; treatment-by-smoking interaction P = 0.03).
In advanced EGFR-non-small-cell lung cancer patients, the addition of an angiogenesis inhibitor to EGFR-tyrosine kinase inhibitor therapy provides a statistically significant PFS and OS benefit in smokers, but not in non-smokers. The biological basis for this observation should be pursued and could determine whether this might be due to a specific co-mutational pattern produced by tobacco exposure.
ETOP 10-16 BOOSTER 试验未能证明在二线治疗中添加贝伐珠单抗可使奥希替尼无进展生存期(PFS)获益。然而,一项探索性亚组分析表明,该联合治疗对有吸烟史的患者具有 PFS 获益,并促使我们开展了这项研究。
按照系统评价和荟萃分析的首选报告项目进行了一项系统评价和荟萃分析,以评估在表皮生长因子受体(EGFR)酪氨酸激酶抑制剂治疗中添加血管生成抑制剂对吸烟状态的影响。根据发表在主要肿瘤大会上或截至 2021 年 11 月 1 日在 PubMed 上的研究,使用了所有相关的随机对照试验。主要关注根据吸烟状态评估的 PFS,其次是总生存期(OS)。通过固定或随机效应模型估算了合并和交互风险比(HR),具体取决于检测到的异质性程度。使用修订后的 Cochrane 随机对照试验偏倚评估工具(RoB 2)评估偏倚。
有 1291 名患者的 PFS(7 项研究)和 678 名患者的 OS(4 项研究)提供了有关吸烟的信息。所有研究的偏倚风险均较低。联合治疗显著延长了吸烟者的 PFS [n=502,HR=0.55,95%置信区间(CI):0.44-0.69],但对不吸烟者无显著影响(n=789,HR=0.92,95%CI:0.66-1.27;治疗-吸烟交互作用 P=0.02)。同样,对于吸烟者(n=271,HR=0.66,95%CI:0.47-0.93),而非不吸烟者(n=407,HR=1.07,95%CI:0.82-1.42;治疗-吸烟交互作用 P=0.03),联合治疗显著延长了 OS。
在晚期 EGFR 非小细胞肺癌患者中,EGFR 酪氨酸激酶抑制剂联合血管生成抑制剂治疗可显著提高吸烟者的 PFS 和 OS,但不提高不吸烟者的 PFS 和 OS。应该进一步研究这种观察结果的生物学基础,这可能决定其是否归因于烟草暴露引起的特定共突变模式。