Department of Anesthesiology, Stomatological Hospital of Chongqing Medical University, 426 Songshi North Road, Yubei District, Chongqing, China.
Chongqing Key Laboratory of Oral Diseases and Biomedical Sciences, Chongqing, China.
Paediatr Drugs. 2022 Jul;24(4):413-421. doi: 10.1007/s40272-022-00510-5. Epub 2022 Jun 13.
Emergence delirium can occur after general anesthesia in children. An intravenous infusion of alfentanil may reduce the incidence or severity of emergence delirium after sevoflurane anesthesia.
The study aimed to investigate the effects of alfentanil intravenous infusion on emergence delirium and other perioperative complications.
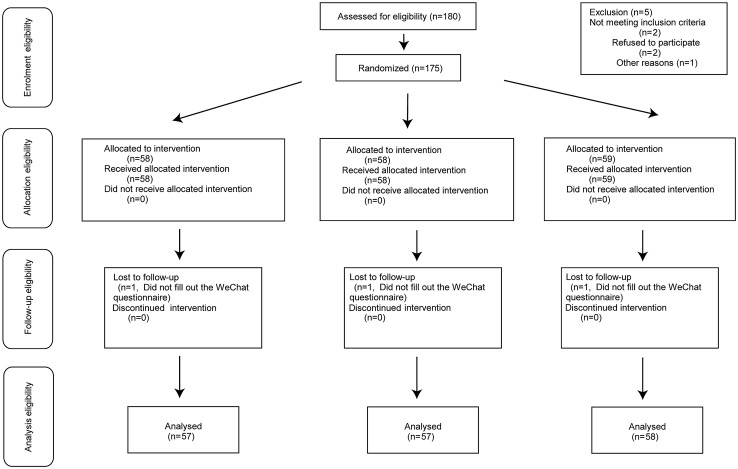
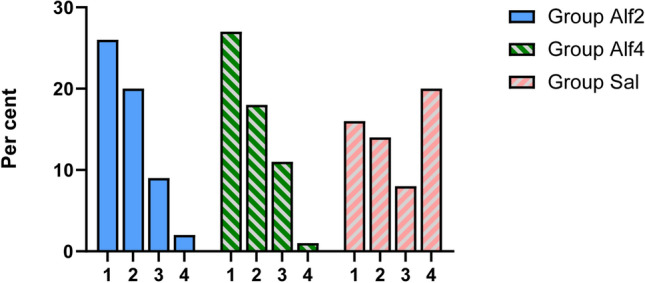
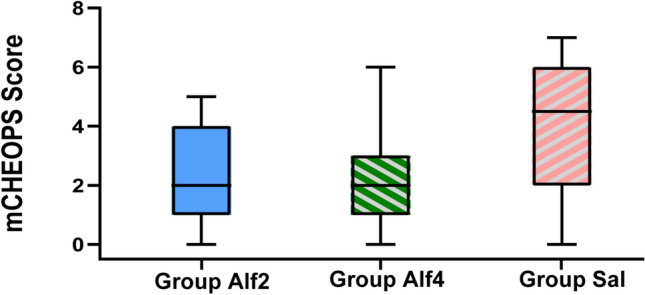
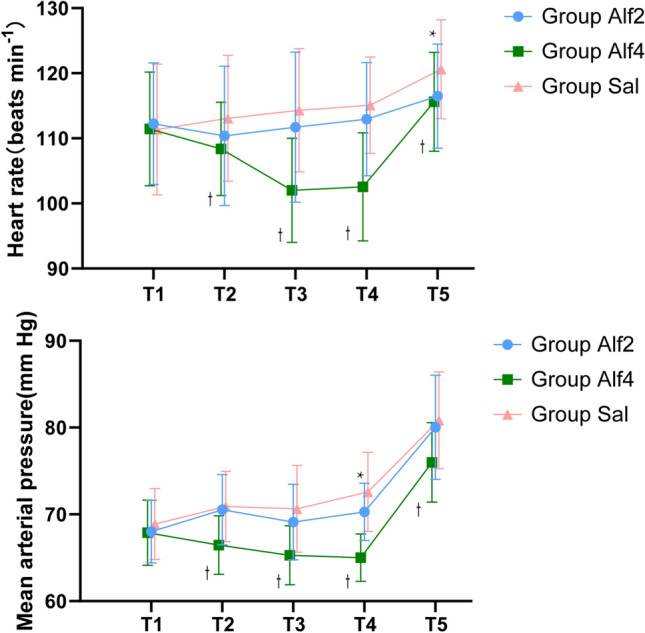
This was a single-center, randomized, placebo-controlled, double-blind clinical trial. A total of 172 children undergoing ambulatory dental treatment were randomized into three groups. Alfentanil group Alf2 received 0.2 μg/kg/min of alfentanil for continuous infusion, alfentanil group Alf4 received 0.4 μg/kg/min alfentanil, and the saline group (group Sal) received a continuous infusion of normal saline, with the same volume as the two other groups, as a placebo. The incidence of emergence delirium (assessed by the Paediatric Anaesthesia Emergence Delirium [PAED] scale), hemodynamic parameters, and recovery characteristics were recorded during the recovery period. The Aono scale was also used to assess for emergence delirium. A WeChat applet was designed to facilitate a caregiver teleconsultation and to provide feedback on postoperative nausea and vomiting and any other complications after discharge.
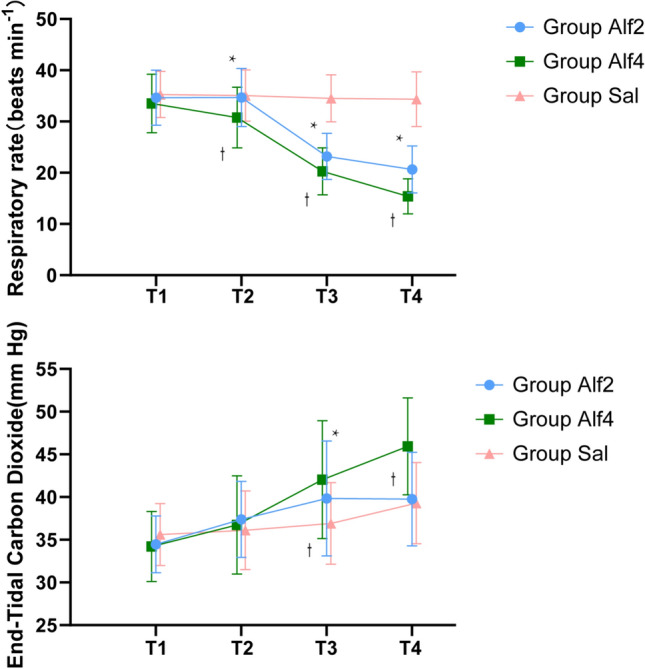
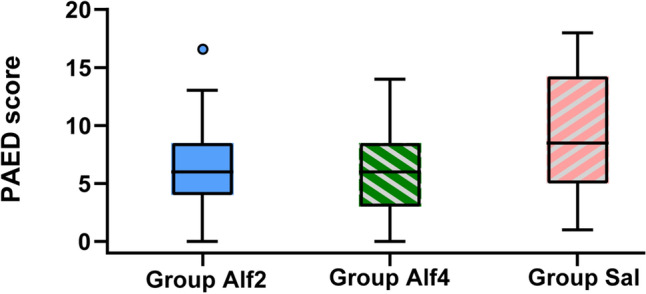
The incidence of emergence delirium in group Alf2 (22.9%) and group Alf4 (21.1%) was significantly lower than that observed in the Sal group (48.3%). The PAED scores in group Alf2 (6.4 ± 3.5) and group Alf4 (5.8 ± 3.8) were significantly lower than those for group Sal (9.6 ± 5.1) (p < 0.01). Ten children in the Alf4 group needed manual ventilatory assistance to maintain end-tidal carbon dioxide (ETCO) < 55 mm; children in group Alf2 did not. There was no significant difference between the discharge time of groups Alf2 and Sal (31.2 ± 4.64 vs 30.5 ± 2.82 min; 0.659 [95% confidence interval {CI} -1.052 to 2.369], p = 0.643); the time to discharge of group Alf4 (35.16 ± 3.97 min) was significantly longer than that of groups Alf2 and Sal (p < 0.01). The incidence of nausea and vomiting was similar in the three groups. No other clinically relevant adverse events were observed.
Intravenous infusion of 0.2 μg/kg/min and 0.4 μg/kg/min alfentanil decreased the incidence of emergence delirium in the post-anesthesia care unit. The 0.2 μg/kg/min dose of alfentanil resulted in less respiratory depression and discharge delay than the 0.4 μg/kg/min alfentanil dose.
Chinese Clinical Trial Registry (ChiCTR2100043320).
全身麻醉后儿童可能会出现苏醒期谵妄。舒芬太尼麻醉后静脉输注阿芬太尼可能会降低苏醒期谵妄的发生率或严重程度。
本研究旨在探讨阿芬太尼静脉输注对苏醒期谵妄及其他围手术期并发症的影响。
这是一项单中心、随机、安慰剂对照、双盲临床试验。共纳入 172 例行日间牙科治疗的儿童,随机分为三组。阿芬太尼组 Alf2 接受 0.2μg/kg/min 的阿芬太尼持续输注,阿芬太尼组 Alf4 接受 0.4μg/kg/min 的阿芬太尼,生理盐水组(Sal 组)接受与其他两组相同体积的生理盐水作为安慰剂。记录恢复期苏醒期谵妄(采用小儿麻醉苏醒期谵妄量表评估)、血流动力学参数和恢复特征。还使用 Aono 量表评估苏醒期谵妄。设计了一个微信小程序,方便照顾者远程咨询,并提供术后恶心呕吐和出院后任何其他并发症的反馈。
Alf2 组(22.9%)和 Alf4 组(21.1%)的苏醒期谵妄发生率明显低于 Sal 组(48.3%)。Alf2 组(6.4±3.5)和 Alf4 组(5.8±3.8)的 PAED 评分明显低于 Sal 组(9.6±5.1)(p<0.01)。Alf4 组 10 例患儿需要手动通气辅助以维持呼气末二氧化碳(ETCO)<55mmHg;Alf2 组患儿不需要。Alf2 组和 Sal 组的出院时间无显著差异(31.2±4.64 vs 30.5±2.82 min;0.659[95%置信区间(CI)-1.052 至 2.369],p=0.643);Alf4 组(35.16±3.97 min)的出院时间明显长于 Alf2 组和 Sal 组(p<0.01)。三组恶心呕吐的发生率相似。未观察到其他有临床意义的不良事件。
舒芬太尼麻醉后静脉输注 0.2μg/kg/min 和 0.4μg/kg/min 的阿芬太尼可降低麻醉后复苏室苏醒期谵妄的发生率。阿芬太尼 0.2μg/kg/min 的剂量导致呼吸抑制和出院延迟的发生率低于 0.4μg/kg/min 的阿芬太尼剂量。
中国临床试验注册中心(ChiCTR2100043320)。