Division of Epilepsy, Department of Neurology, Mayo Clinic, Rochester, Minnesota, USA.
Epilepsy Center, University Medical Center-University of Freiburg, Freiburg, Germany.
Epilepsia. 2022 Oct;63(10):2445-2460. doi: 10.1111/epi.17329. Epub 2022 Aug 9.
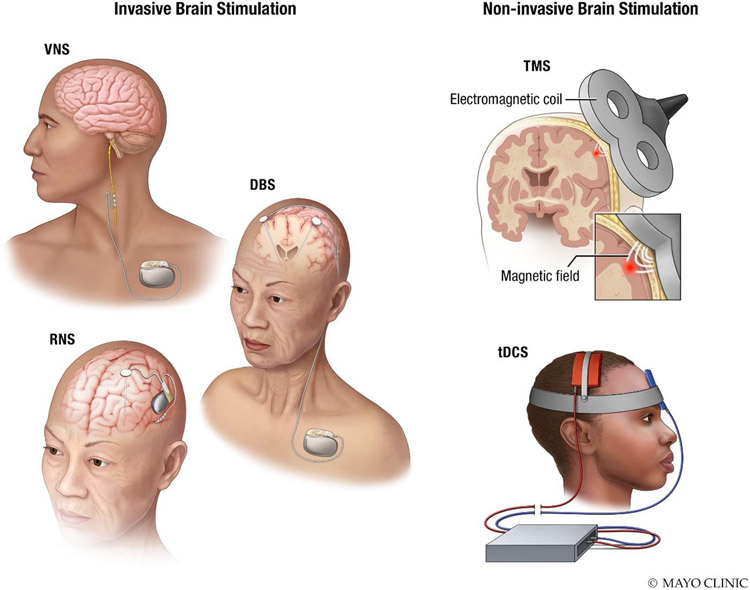
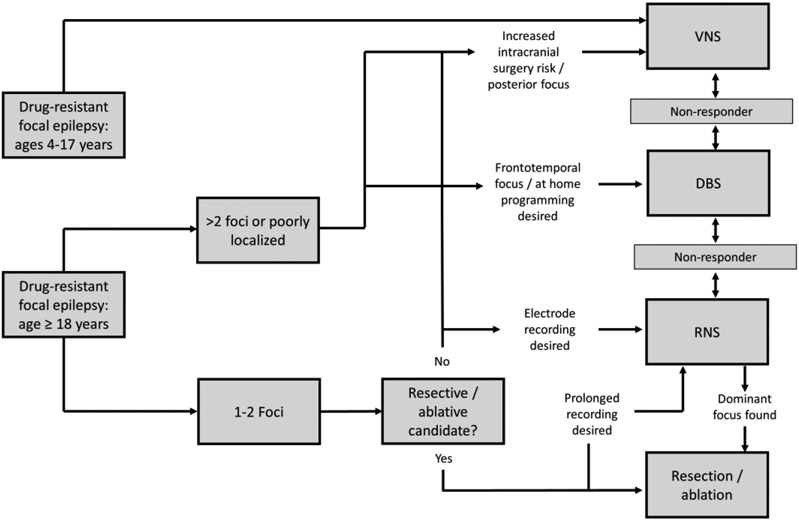
Neuromodulation is a key therapeutic tool for clinicians managing patients with drug-resistant epilepsy. Multiple devices are available with long-term follow-up and real-world experience. The aim of this review is to give a practical summary of available neuromodulation techniques to guide the selection of modalities, focusing on patient selection for devices, common approaches and techniques for initiation of programming, and outpatient management issues. Vagus nerve stimulation (VNS), deep brain stimulation of the anterior nucleus of the thalamus (DBS-ANT), and responsive neurostimulation (RNS) are all supported by randomized controlled trials that show safety and a significant impact on seizure reduction, as well as a suggestion of reduction in the risk of sudden unexplained death in epilepsy (SUDEP). Significant seizure reductions are observed after 3 months for DBS, RNS, and VNS in randomized controlled trials, and efficacy appears to improve with time out to 7 to 10 years of follow-up for all modalities, albeit in uncontrolled follow-up or retrospective studies. A significant number of patients experience seizure-free intervals of 6 months or more with all three modalities. Number and location of epileptogenic foci are important factors affecting efficacy, and together with comorbidities such as severe mood or sleep disorders, may influence the choice of modality. Programming has evolved-DBS is typically initiated at lower current/voltage than used in the pivotal trial, whereas target charge density is lower with RNS, however generalizable optimal parameters are yet to be defined. Noninvasive brain stimulation is an emerging stimulation modality, although it is currently not used widely. In summary, clinical practice has evolved from those established in pivotal trials. Guidance is now available for clinicians who wish to expand their approach, and choice of neuromodulation technique may be tailored to individual patients based on their epilepsy characteristics, risk tolerance, and preferences.
神经调节是管理耐药性癫痫患者的临床医生的重要治疗工具。有多种设备可供使用,具有长期随访和真实世界的经验。本综述的目的是提供可用的神经调节技术的实用总结,以指导选择方式,重点是为设备选择患者,常见的启动编程方法和技术,以及门诊管理问题。迷走神经刺激(VNS)、丘脑前核深部脑刺激(DBS-ANT)和反应性神经刺激(RNS)均得到随机对照试验的支持,这些试验表明安全性和对减少癫痫发作有显著影响,并提示减少癫痫猝死(SUDEP)的风险。在随机对照试验中,DBS、RNS 和 VNS 在 3 个月后观察到显著的癫痫发作减少,并且在所有治疗方式中,疗效似乎随着时间的推移而改善,最长可达 7 至 10 年的随访时间,但在无对照随访或回顾性研究中。大量患者使用所有三种方式都能达到 6 个月或更长时间的无癫痫发作间隔。癫痫灶的数量和位置是影响疗效的重要因素,与严重的情绪或睡眠障碍等合并症一起,可能会影响治疗方式的选择。编程已经发展——DBS 的初始电流/电压通常低于关键试验中的电流/电压,而 RNS 的目标电荷密度较低,但尚未定义可推广的最佳参数。非侵入性脑刺激是一种新兴的刺激方式,尽管目前尚未广泛使用。总之,临床实践已经从关键试验中发展而来。现在有指南可供希望扩大治疗方法的临床医生使用,并且可以根据患者的癫痫特征、风险承受能力和偏好,为每位患者量身定制神经调节技术的选择。