Salami Pariya, Paulk Angelique C, Soper Daniel J, Bourdillon Pierre, Hadar Peter N, Alamoudi Omar A, Sisterson Nathaniel D, Richardson R Mark, Pati Sandipan, Cash Sydney S
Department of Neurology, Massachusetts General Hospital and Harvard Medical School, Boston, MA, USA.
Department of Neurology, Center for Neurotechnology and Neurorecovery, Massachusetts General Hospital, Boston, MA, USA.
Commun Med (Lond). 2025 May 22;5(1):190. doi: 10.1038/s43856-025-00920-9.
Thalamic stimulation is a promising approach to controlling seizures in patients with intractable epilepsy. It does not, however, provide good control for everyone. A big issue is that the role of the thalamus in seizure organization and propagation is unclear. When using responsive stimulation devices, they must detect seizure activity before sending stimulation. So, it's important to know which parts of the thalamus are involved in different seizures.
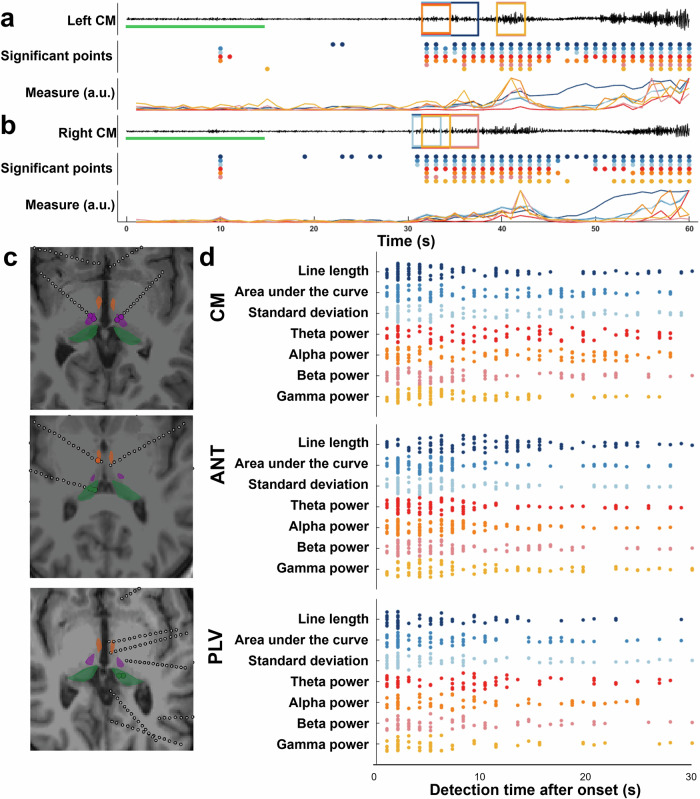
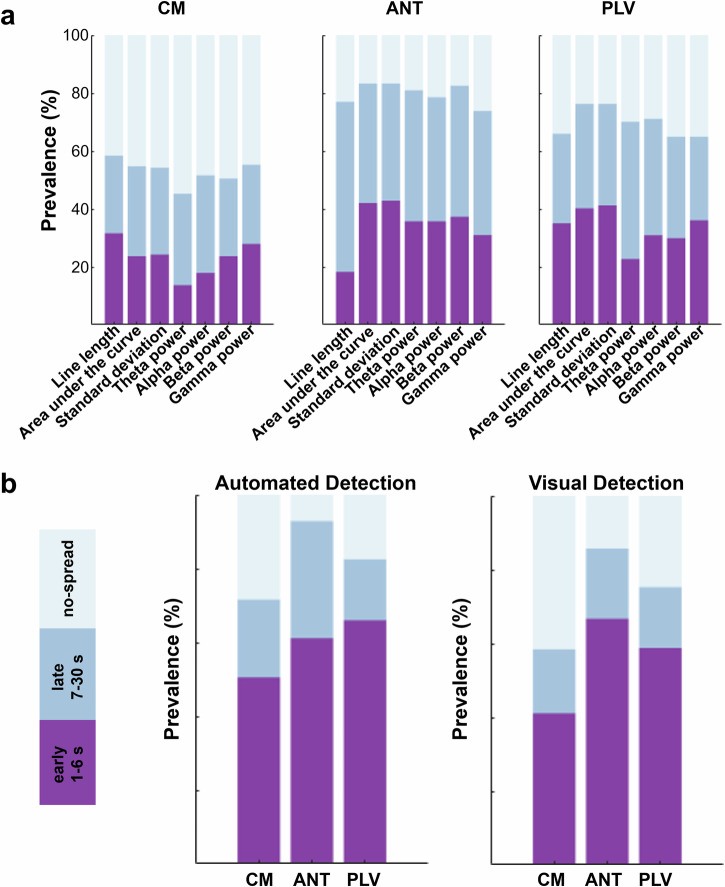
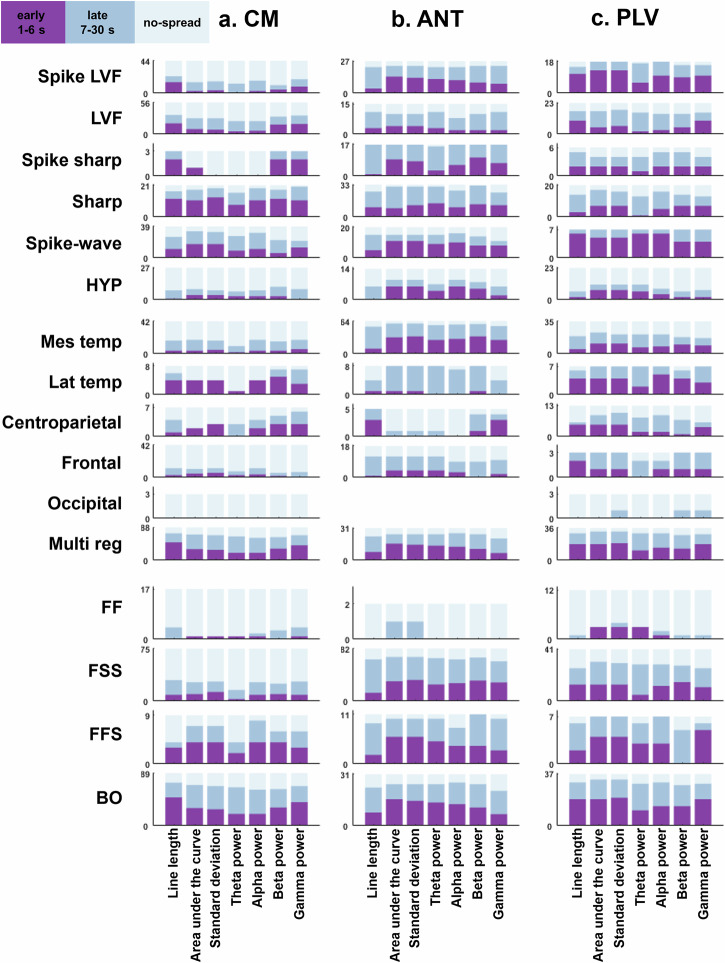
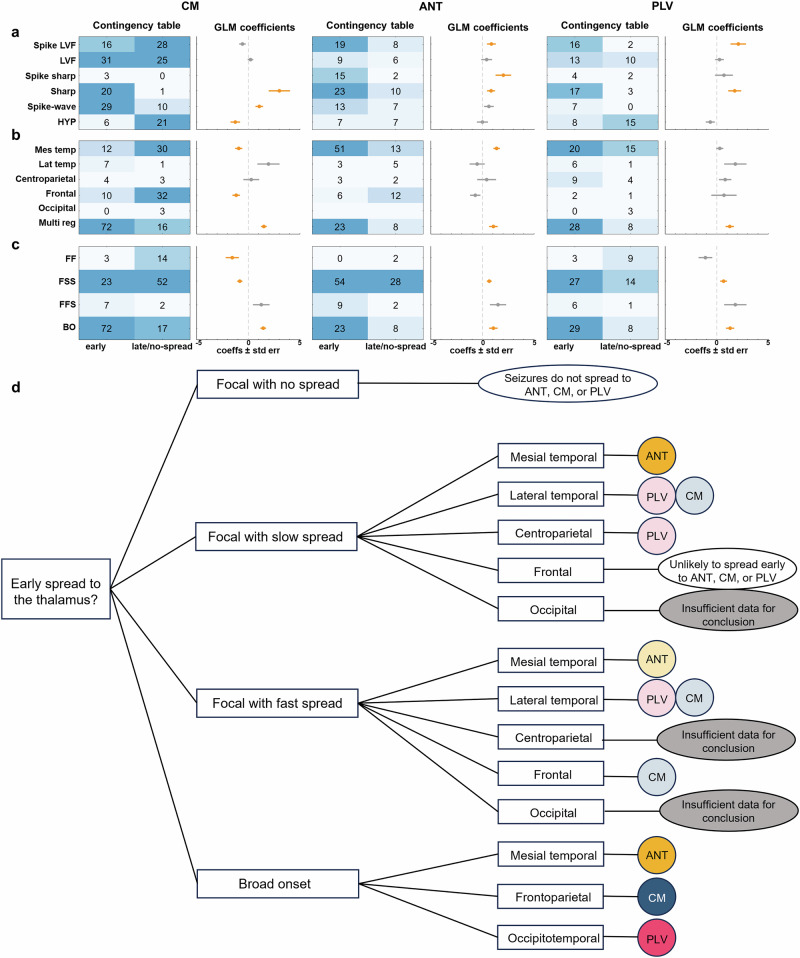
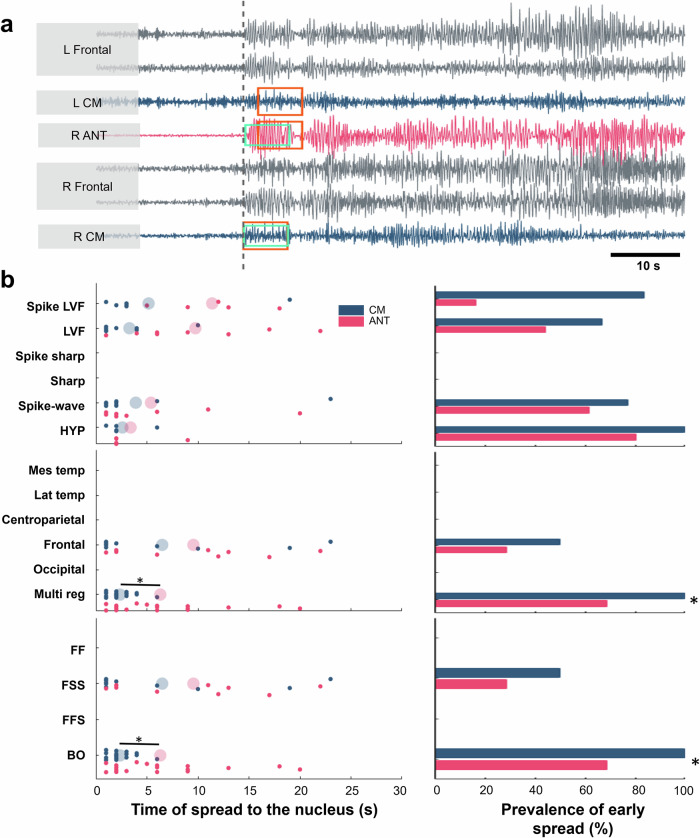
To better choose thalamic targets for stimulation, we studied how different seizures spread to each stimulation target. Expert reviews and automated tools were used to identify seizure spread recorded from invasive recordings. We categorized seizures based on how they start and spread, and determined whether seizures reached thalamic areas early or late. We used generalized linear models (GLM) to evaluate which seizure properties are predictive of time of spread to the thalamus, testing effect significance using Wald tests.
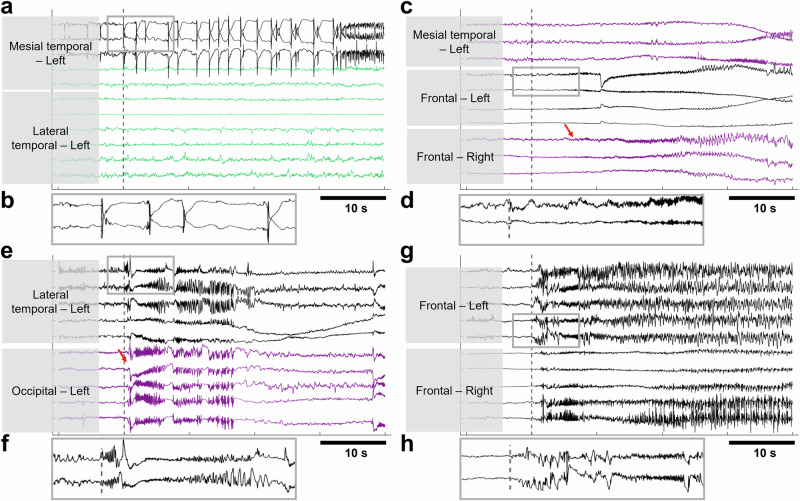
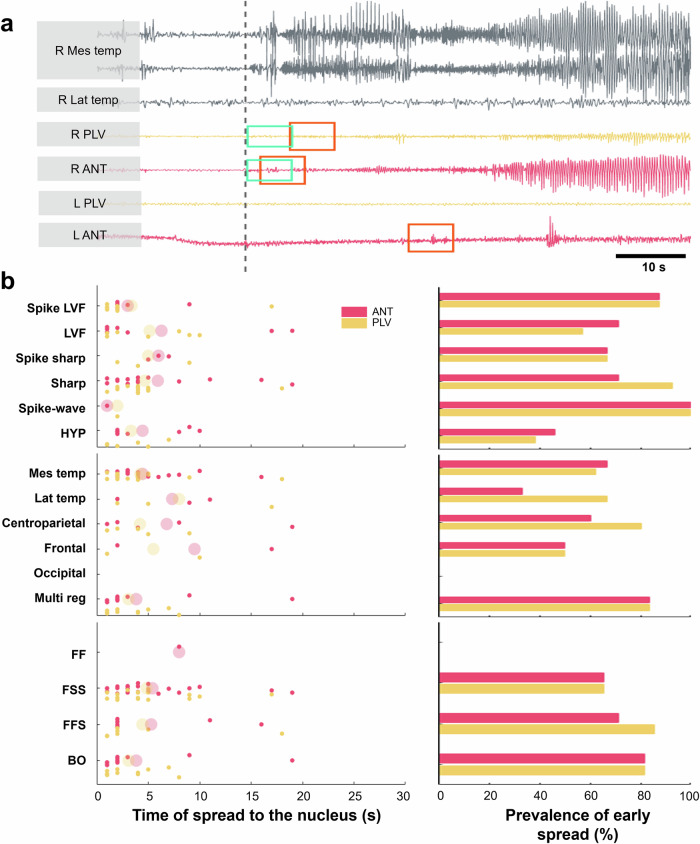
We show that seizures with <2 Hz synchronized-spiking patterns do not spread early to the thalamus, while seizures starting with faster activity (<20 Hz) spread early to all thalamic areas. Most importantly, seizures that begin broadly across the brain quickly recruit the centromedian and pulvinar areas, suggesting these may be better stimulation targets in such cases. Alternatively, seizures that start deep in the temporal lobe tend to involve the anterior part of the thalamus, meaning the centromedian might not be the best choice for those seizures.
Our results suggest that by analyzing electrical activity during seizures, we can better predict which parts of the thalamus are involved. This could lead to more effective stimulation treatments for people with epilepsy.
丘脑刺激是控制难治性癫痫患者癫痫发作的一种有前景的方法。然而,它并非对所有人都能提供良好的控制效果。一个大问题是丘脑在癫痫发作的组织和传播中的作用尚不清楚。在使用响应性刺激设备时,它们必须在发送刺激之前检测到癫痫活动。因此,了解丘脑的哪些部分参与不同的癫痫发作很重要。
为了更好地选择丘脑刺激靶点,我们研究了不同的癫痫发作如何扩散到每个刺激靶点。使用专家评审和自动化工具来识别从侵入性记录中记录到的癫痫发作扩散情况。我们根据癫痫发作的起始和扩散方式对其进行分类,并确定癫痫发作是早期还是晚期到达丘脑区域。我们使用广义线性模型(GLM)来评估哪些癫痫发作特征可预测扩散到丘脑的时间,并使用Wald检验来检验效应的显著性。
我们发现,同步尖峰模式频率<2Hz的癫痫发作不会早期扩散到丘脑,而起始活动较快(<20Hz)的癫痫发作会早期扩散到所有丘脑区域。最重要的是,在整个大脑广泛起始的癫痫发作会迅速累及中央中核和丘脑枕区域,这表明在这种情况下这些区域可能是更好的刺激靶点。或者,起源于颞叶深部的癫痫发作往往会累及丘脑前部,这意味着中央中核可能不是这些癫痫发作的最佳选择。
我们的结果表明,通过分析癫痫发作期间的电活动,我们可以更好地预测丘脑的哪些部分受到累及。这可能会为癫痫患者带来更有效的刺激治疗。