Genomic Epidemiology Branch, International Agency for Research on Cancer, Lyon, France.
Division of Infections and Cancer Epidemiology, German Cancer Research Center (DKFZ), Heidelberg, Germany.
J Clin Oncol. 2022 Nov 1;40(31):3613-3622. doi: 10.1200/JCO.21.01785. Epub 2022 Jun 14.
Seropositivity for the HPV16-E6 oncoprotein is a promising marker for early detection of oropharyngeal cancer (OPC), but the absolute risk of OPC after a positive or negative test is unknown.
We constructed an OPC risk prediction model that integrates (1) relative odds of OPC for HPV16-E6 serostatus and cigarette smoking from the human papillomavirus (HPV) Cancer Cohort Consortium (HPVC3), (2) US population risk factor data from the National Health Interview Survey, and (3) US sex-specific population rates of OPC and mortality.
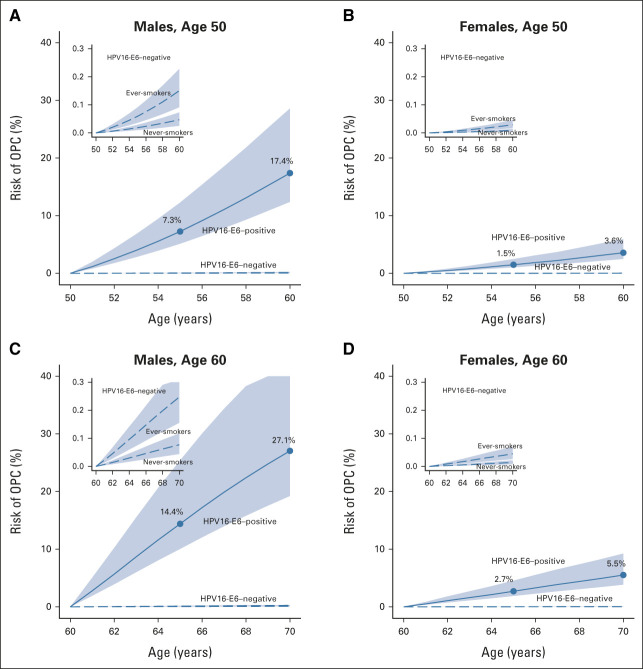
The nine HPVC3 cohorts included 365 participants with OPC with up to 10 years between blood draw and diagnosis and 5,794 controls. The estimated 10-year OPC risk for HPV16-E6 seropositive males at age 50 years was 17.4% (95% CI, 12.4 to 28.6) and at age 60 years was 27.1% (95% CI, 19.2 to 45.4). Corresponding 5-year risk estimates were 7.3% and 14.4%, respectively. For HPV16-E6 seropositive females, 10-year risk estimates were 3.6% (95% CI, 2.5 to 5.9) at age 50 years and 5.5% (95% CI, 3.8 to 9.2) at age 60 years and 5-year risk estimates were 1.5% and 2.7%, respectively. Over 30 years, after a seropositive result at age 50 years, an estimated 49.9% of males and 13.3% of females would develop OPC. By contrast, 10-year risks among HPV16-E6 seronegative people were very low, ranging from 0.01% to 0.25% depending on age, sex, and smoking status.
We estimate that a substantial proportion of HPV16-E6 seropositive individuals will develop OPC, with 10-year risks of 17%-27% for males and 4%-6% for females age 50-60 years in the United States. This high level of risk may warrant periodic, minimally invasive surveillance after a positive HPV16-E6 serology test, particularly for males in high-incidence regions. However, an appropriate clinical protocol for surveillance remains to be established.
HPV16-E6 癌蛋白的血清阳性是口咽癌(OPC)早期检测的一个有前途的标志物,但 HPV16-E6 检测阳性或阴性后的 OPC 绝对风险尚不清楚。
我们构建了一个 OPC 风险预测模型,该模型整合了(1)HPV 癌症队列联盟(HPVCC3)中 HPV16-E6 血清状态和吸烟对 OPC 的相对优势比,(2)来自国家健康访谈调查的美国人口风险因素数据,以及(3)美国特定性别 OPC 和死亡率的人口率。
HPVCC3 共有 9 个队列,包括 365 名 OPC 患者,从采血到诊断的时间长达 10 年,5794 名对照者。在 50 岁时,HPV16-E6 血清阳性男性的 10 年 OPC 风险估计值为 17.4%(95%CI,12.4%至 28.6%),60 岁时为 27.1%(95%CI,19.2%至 45.4%)。相应的 5 年风险估计值分别为 7.3%和 14.4%。对于 HPV16-E6 血清阳性的女性,50 岁时 10 年风险估计值为 3.6%(95%CI,2.5%至 5.9%),60 岁时为 5.5%(95%CI,3.8%至 9.2%),5 年风险估计值分别为 1.5%和 2.7%。在 30 多年的时间里,50 岁时 HPV16-E6 血清阳性的结果后,估计有 49.9%的男性和 13.3%的女性会患上 OPC。相比之下,HPV16-E6 血清阴性者的 10 年风险非常低,取决于年龄、性别和吸烟状况,范围在 0.01%至 0.25%之间。
我们估计,相当一部分 HPV16-E6 血清阳性者将发展为 OPC,美国 50-60 岁男性的 10 年风险为 17%-27%,女性为 4%-6%。这种高风险可能需要在 HPV16-E6 血清学检测呈阳性后定期进行微创监测,尤其是在高发病率地区的男性中。然而,适当的临床监测方案仍有待建立。