Department of Thoracic Surgery, Sun Yat-sen University Cancer Center, Guangzhou City, Guangdong Province, China.
State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou City, Guangdong Province, China.
Thorac Cancer. 2022 Aug;13(15):2106-2116. doi: 10.1111/1759-7714.14456. Epub 2022 Jun 15.
To investigate the impact of station 3A lymph node dissection (LND) on overall survival (OS) and disease-free survival (DFS) in completely resected right-side non-small-cell lung cancer (NSCLC) patients.
A total of 1661 cases with completely resected right-side NSCLC were included. Propensity score matching (PSM) was performed to minimize selection bias, and a logistic regression model was conducted to investigate the risk factors associated with station 3A lymph node metastasis (LNM). The Kaplan-Meier method and Cox proportional hazards model were used to evaluate the impact of station 3A LND on survival.
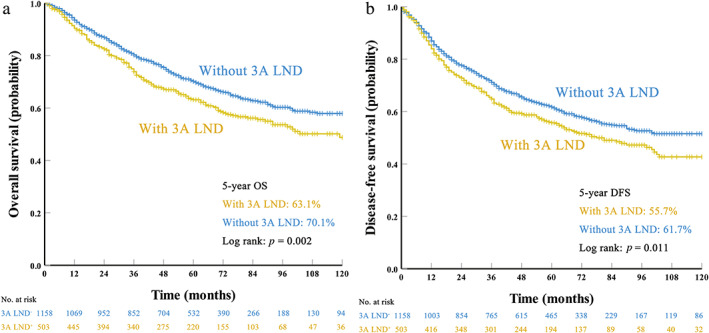
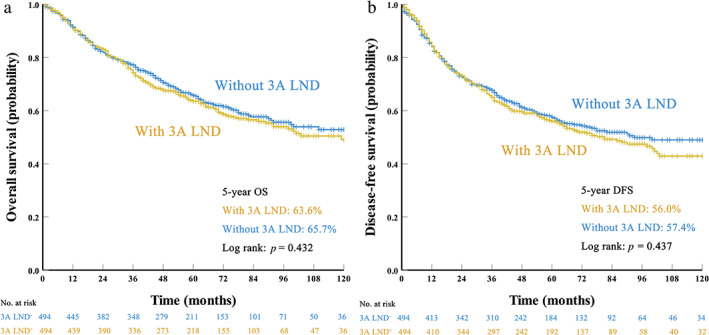
For the entire cohort, 503 patients (30.3%) underwent station 3A LND. Of those, 11.3% (57/503) presented station 3A LNM. Univariate and multivariate logistic analyses showed that station 10 LNM, tumor location, and the number of resected lymph nodes were independent risk factors associated with station 3A LNM. Before PSM, patients with station 3A LND had worse 5-year OS (p = 0.002) and DFS (p = 0.011), and more drainage on postoperative day 1 (p = 0.041) than those without. After PSM, however, station 3A LND was not associated with the 5-year OS (65.7% vs. 63.6%, p = 0.432) or DFS (57.4% vs. 56.0%, p = 0.437). The multivariate analysis further confirmed that station 3A LND was not a prognostic factor (OS, p = 0.361; DFS, p = 0.447).
Station 3A LND could not improve long-term outcomes and it was unnecessary to dissect station 3A lymph nodes during surgery of right-side NSCLC.
探讨完全切除的右侧非小细胞肺癌(NSCLC)患者的 3A 站淋巴结清扫术(LND)对总生存(OS)和无病生存(DFS)的影响。
共纳入 1661 例完全切除的右侧 NSCLC 患者。采用倾向评分匹配(PSM)以最小化选择偏倚,并进行逻辑回归模型以探讨与 3A 站淋巴结转移(LNM)相关的危险因素。采用 Kaplan-Meier 方法和 Cox 比例风险模型评估 3A 站 LND 对生存的影响。
对于整个队列,503 例患者(30.3%)接受了 3A 站 LND。其中,11.3%(57/503)存在 3A 站 LNM。单因素和多因素逻辑分析表明,10 站 LNM、肿瘤位置和切除的淋巴结数量是与 3A 站 LNM 相关的独立危险因素。在 PSM 之前,接受 3A 站 LND 的患者 5 年 OS(p=0.002)和 DFS(p=0.011)较差,术后第 1 天引流更多(p=0.041)。然而,PSM 后,3A 站 LND 与 5 年 OS(65.7% vs. 63.6%,p=0.432)或 DFS(57.4% vs. 56.0%,p=0.437)无关。多因素分析进一步证实,3A 站 LND 不是预后因素(OS,p=0.361;DFS,p=0.447)。
3A 站 LND 不能改善长期预后,右侧 NSCLC 手术时无需解剖 3A 站淋巴结。