Rocco Raffaele, Hendriksen Brandon S, Ortiz Belisario A, Shen K Robert, Cassivi Stephen D, Saddoughi Sahar, Reisenauer Janani S, Wigle Dennis A, Tapias Luis F
Division of Thoracic Surgery, Department of Surgery, Mayo Clinic, Rochester, MN, USA.
J Thorac Dis. 2024 Nov 30;16(11):7663-7674. doi: 10.21037/jtd-24-971. Epub 2024 Nov 11.
The American College of Surgeons Commission on Cancer (CoC) revised operative quality standards recommending resection of lymph nodes from at least one hilar station and three different mediastinal stations in all curative-intent pulmonary resections. This study evaluated the prognostic value and factors associated with adherence to this new CoC standard in patients with resected clinical stage IA non-small cell lung cancer (NSCLC).
Retrospective review of 654 patients who underwent pulmonary resection for clinical IA NSCLC. The study population was divided into patients that met and did not meet the CoC standard.
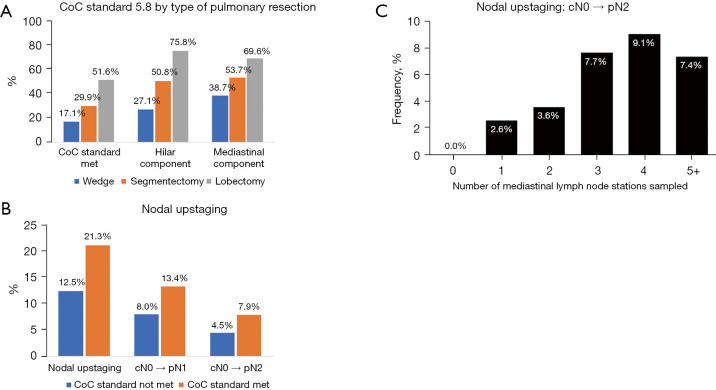
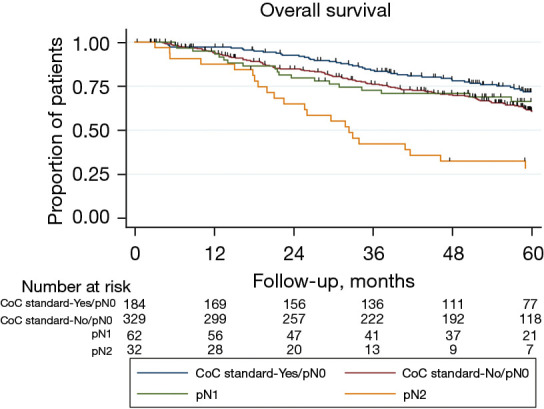
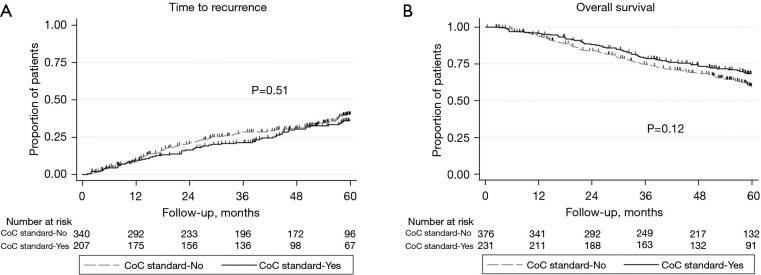
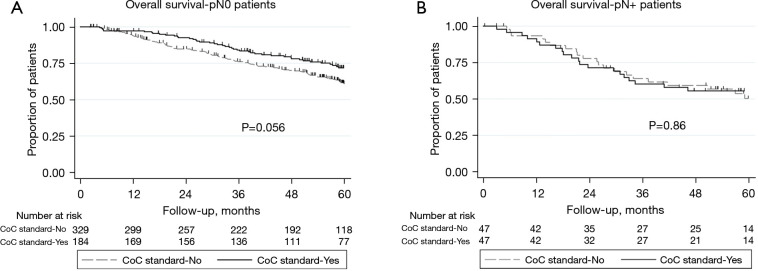
The CoC standard was met in only 254 (38.8%) patients. Factors associated with meeting the CoC standard included left-sided resections, open technique, and type of pulmonary resection. CoC standard was met in 51.6% of lobectomies, 29.9% of segmentectomies, and 17.1% of wedge resections (P<0.001). Nodal upstaging was more frequent in patients meeting the CoC standard (21.3% 12.5% when standard not met; P=0.004). Time to recurrence [adjusted hazard ratio (aHR): 0.86, 95% confidence interval (CI): 0.63-1.17, P=0.33] and overall survival (aHR: 0.78, 95% CI: 0.58-1.05, P=0.10) were not different between CoC standard groups. However, patients not meeting the CoC standard and classified as pN0 exhibited an overall survival that resembled that of patients with pN1 disease.
Left-sided resections, open technique and lobectomy were associated with meeting the CoC standard. However, this standard did not have a significant impact on long-term outcomes. Larger studies with longer follow-up are needed to clarify the role of the CoC standard in patients with resected stage IA NSCLC.
美国外科医师学会癌症委员会(CoC)修订了手术质量标准,建议在所有根治性意图的肺切除术中,至少从一个肺门站和三个不同的纵隔站切除淋巴结。本研究评估了接受手术切除的临床IA期非小细胞肺癌(NSCLC)患者遵守这一新CoC标准的预后价值及相关因素。
回顾性分析654例行临床IA期NSCLC肺切除术的患者。研究人群分为符合和不符合CoC标准的患者。
仅254例(38.8%)患者符合CoC标准。与符合CoC标准相关的因素包括左侧切除术、开放技术和肺切除类型。肺叶切除术患者中51.6%符合CoC标准,肺段切除术患者中29.9%符合,楔形切除术患者中17.1%符合(P<0.001)。符合CoC标准的患者中淋巴结分期上调更常见(符合标准时为21.3%,不符合标准时为12.5%;P=0.004)。CoC标准组之间的复发时间[调整后风险比(aHR):0.86,95%置信区间(CI):0.63 - 1.17,P=0.33]和总生存期(aHR:0.78,95%CI:0.58 - 1.05,P=0.10)无差异。然而,不符合CoC标准且分类为pN0的患者的总生存期与pN1疾病患者相似。
左侧切除术、开放技术和肺叶切除术与符合CoC标准相关。然而,该标准对长期预后没有显著影响。需要进行更大规模、更长随访时间的研究来阐明CoC标准在接受手术切除的IA期NSCLC患者中的作用。