Geirsson Arnar, Owen Clarence H, Binford Robert S, Voeller Rochus K, Burke Christopher R, McNeil Jeffrey D, Wei Lawrence M, Badhwar Vinay, Rankin J Scott
Department of Cardiac Surgery, Yale University School of Medicine, New Haven, Conn.
Cone Health, Greensboro, NC.
JTCVS Tech. 2022 Mar 3;13:26-30. doi: 10.1016/j.xjtc.2022.02.031. eCollection 2022 Jun.
Isolated right coronary leaflet prolapse is a common cause of nonaneurysmal aortic insufficiency, but can rarely occur in patients with proximal aortic aneurysms. Standardized techniques for routine autologous repair of this disorder are presented.
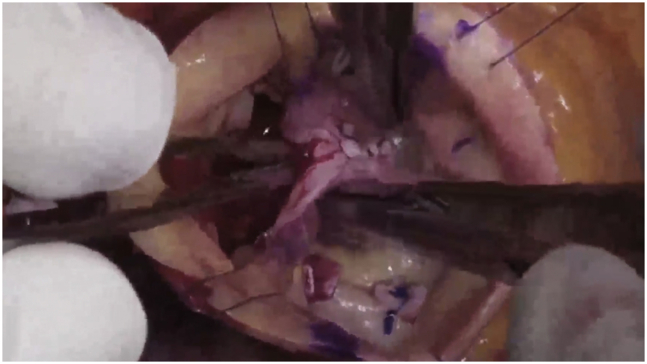
Most aortic valve leaflet prolapse is isolated to the right coronary leaflet, with hypertension and annular dilatation being contributory. Echocardiographically, a posteriorly eccentric aortic insufficiency jet together with "fracture" of the right leaflet tip are diagnostic. Primary repair includes internal geometric ring annuloplasty to downsize and reshape the annulus, together with central plication of the prolapsing leaflet. Thickened, scarred, or retracted noduli are released using an ultrasonic aspirator. The goal is to achieve equivalent coaptation heights of ≥8 mm for all 3 leaflets.
Three videos of 6 cases are provided to illustrate these techniques. In the first, 3 patients are shown with classic isolated right leaflet prolapse. In the second and third videos, alternative pathologies are presented for contrast. Applying the reconstructive approaches of geometric ring annuloplasty, leaflet plication, and ultrasonic nodular release, excellent early and late repair outcomes are obtainable in most patients.
The combination of aortic ring annuloplasty, central leaflet plication, and ultrasonic nodular release allows routine and standardized repair of right coronary leaflet prolapse, either isolated or concomitant with aneurysm surgery.
孤立性右冠状动脉瓣叶脱垂是导致非动脉瘤性主动脉瓣关闭不全的常见原因,但在近端主动脉瘤患者中很少见。本文介绍了针对该疾病进行常规自体修复的标准化技术。
大多数主动脉瓣叶脱垂局限于右冠状动脉瓣叶,高血压和瓣环扩张是促成因素。超声心动图检查时,后偏心性主动脉瓣关闭不全喷射以及右瓣叶尖端“断裂”具有诊断意义。初次修复包括进行内部几何环形瓣环成形术以缩小和重塑瓣环,同时对脱垂瓣叶进行中央折叠。使用超声吸引器松解增厚、瘢痕化或回缩的小结节。目标是使所有三个瓣叶的对合高度达到≥8毫米。
提供了6例患者的3个视频以说明这些技术。第一个视频展示了3例典型的孤立性右瓣叶脱垂患者。在第二个和第三个视频中,展示了其他病变情况以作对比。应用几何环形瓣环成形术、瓣叶折叠和超声小结节松解的重建方法,大多数患者可获得良好的早期和晚期修复效果。
主动脉瓣环成形术、中央瓣叶折叠和超声小结节松解相结合,可对孤立性或与动脉瘤手术同时存在的右冠状动脉瓣叶脱垂进行常规和标准化修复。