Department of Molecular Medicine , University of Southern Denmark , Odense , Denmark.
Liver Research Group , Department of Gastroenterology and Hepatology , University Hospital of South Denmark , Esbjerg , Denmark.
Hepatology. 2023 Feb 1;77(2):558-572. doi: 10.1002/hep.32620. Epub 2022 Jul 14.
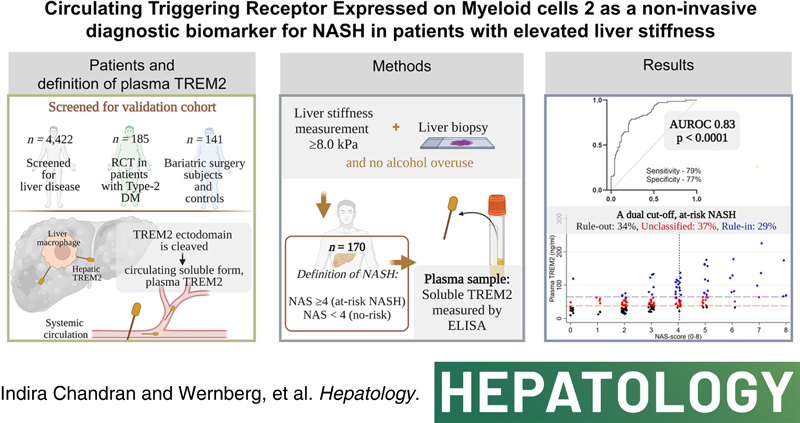
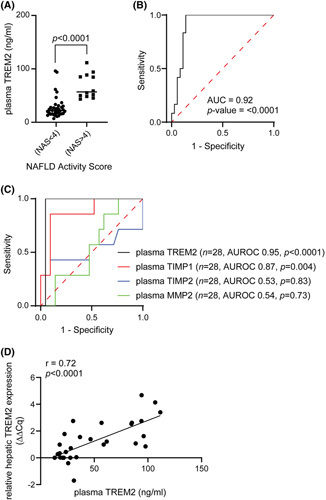
Reliable noninvasive biomarkers are an unmet clinical need for the diagnosis of NASH. This study investigates the diagnostic accuracy of the circulating triggering receptor expressed on myeloid cells 2 (plasma TREM2) as a biomarker for NASH in patients with NAFLD and elevated liver stiffness.
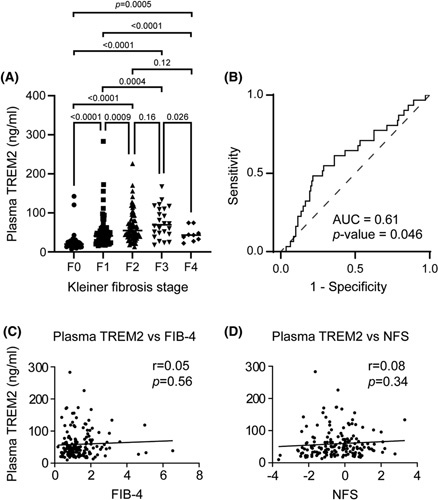
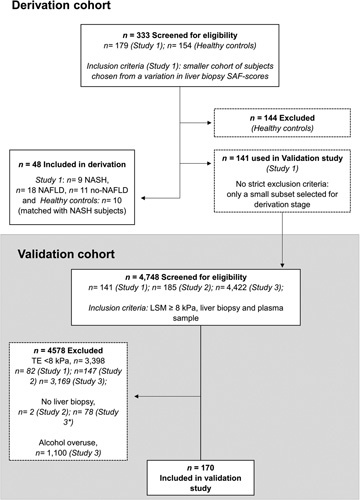
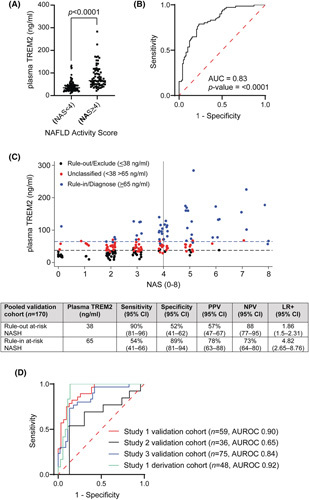
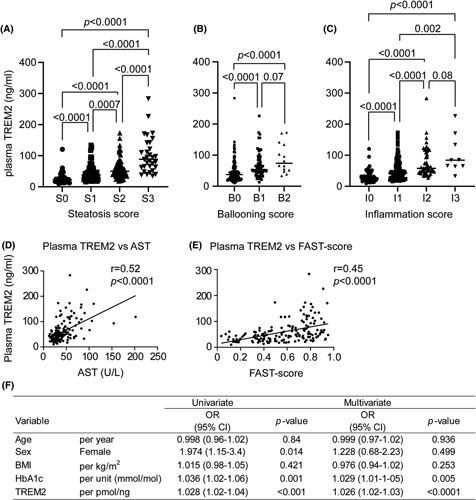
We collected cross-sectional, clinical data including liver biopsies from a derivation ( n = 48) and a validation cohort ( n = 170) of patients with elevated liver stiffness measurement (LSM ≥ 8.0 kPa). Patients with NAFLD activity scores (NAS) ≥4 were defined as having NASH. Plasma TREM2 levels were significantly elevated in patients with NASH of the derivation cohort, with an area under the receiver operating characteristics curve (AUROC) of 0.92 (95% confidence interval [CI], 0.84-0.99). In the validation cohort, plasma TREM2 level increased approximately two-fold in patients with NASH, and a strong diagnostic accuracy was confirmed (AUROC, 0.83; 95% CI, 0.77-0.89; p < 0.0001). Plasma TREM2 levels were associated with the individual histologic features of NAS: steatosis, lobular inflammation, and ballooning ( p < 0.0001), but only weakly with fibrosis stages. Dual cutoffs for rule-in and rule-out were explored: a plasma TREM2 level of ≤38 ng/ml was found to be an optimal NASH rule-out cutoff (sensitivity 90%; specificity 52%), whereas a plasma TREM2 level of ≥65 ng/ml was an optimal NASH rule-in cutoff (specificity 89%; sensitivity 54%).
Plasma TREM2 is a plausible individual biomarker that can rule-in or rule-out the presence of NASH with high accuracy and thus has the potential to reduce the need for liver biopsies and to identify patients who are eligible for clinical trials in NASH.
可靠的非侵入性生物标志物是目前诊断 NASH 的临床需求。本研究旨在探讨髓系细胞触发受体 2(TREM2)在非酒精性脂肪性肝病(NAFLD)伴肝硬度升高患者中的循环水平作为 NASH 生物标志物的诊断准确性。
我们收集了包括肝脏活检在内的横断面临床数据,这些数据来自一个衍生队列(n = 48)和一个验证队列(n = 170),这些患者的肝硬度测量值(LSM)升高(≥8.0 kPa)。NAFLD 活动评分(NAS)≥4 的患者被定义为患有 NASH。衍生队列中 NASH 患者的 TREM2 水平明显升高,其受试者工作特征曲线(ROC)下面积(AUROC)为 0.92(95%置信区间[CI],0.84-0.99)。在验证队列中,NASH 患者的 TREM2 水平增加了约两倍,确认了其具有很强的诊断准确性(AUROC,0.83;95%CI,0.77-0.89;p < 0.0001)。TREM2 水平与 NAS 的个体组织学特征相关:脂肪变性、小叶炎症和气球样变(p < 0.0001),但与纤维化阶段的相关性较弱。探索了 TREM2 水平的双截断值用于排除或确诊 NASH:TREM2 水平≤38 ng/ml 是排除 NASH 的最佳截断值(敏感性 90%;特异性 52%),而 TREM2 水平≥65 ng/ml 是确诊 NASH 的最佳截断值(特异性 89%;敏感性 54%)。
TREM2 是一种有前途的个体生物标志物,可高度准确地排除或确诊 NASH,因此有可能减少肝活检的需求,并确定适合 NASH 临床试验的患者。