Malige Ajith, Beck Matthew, Mun Frederick, Goss Maddie, Boateng Henry, Nwachuku Chinenye
Orthopaedic Surgery, St. Luke's University Health Network, Bethlehem, USA.
Orthopaedic Surgery, Philadelphia College of Osteopathic Medicine, Philadelphia, USA.
Cureus. 2022 May 17;14(5):e25063. doi: 10.7759/cureus.25063. eCollection 2022 May.
While biomechanical and clinical studies detailing the equivalence and, sometimes, the superiority of cerclage wiring fixation compared to plate fixation in select fractures (Vancouver B1 and C) exist, no studies exist detailing outcomes after cerclage wiring fixation in all Vancouver B fracture types. This study explores whether there is a difference in clinical outcomes between Vancouver B fractures fixed with cerclage wiring and those without.
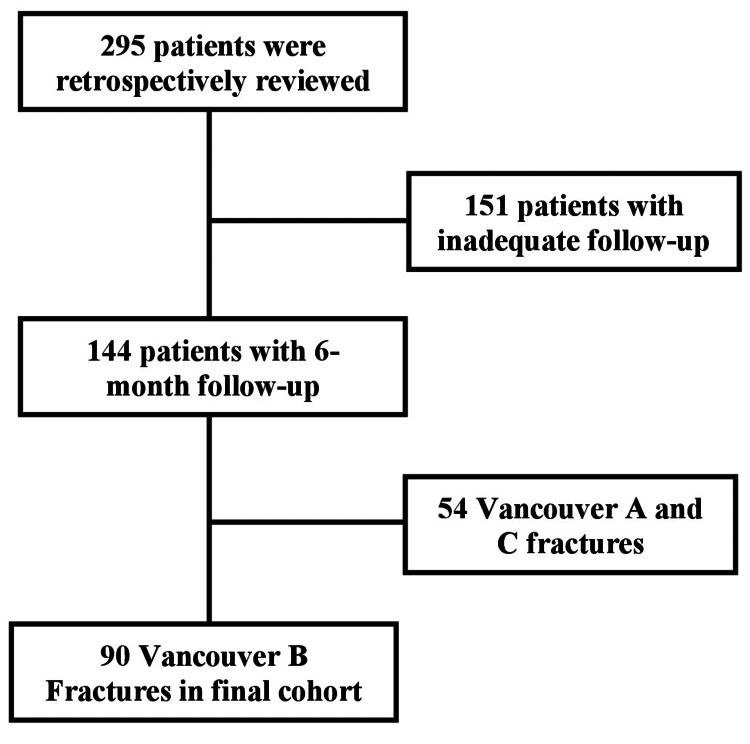
This retrospective multicenter study reviewed 295 patients from 2007 to 2018 with periprosthetic femur fractures. Vancouver B periprosthetic fractures stabilized utilizing cerclage wiring were identified and compared against fractures stabilized without cerclage wiring, with 33% being B1, 48.4% B2, and 18.6% B3 fractures. Demographics, injury details, fracture classification, surgical details, fracture union, and postoperative complications were recorded for each patient.
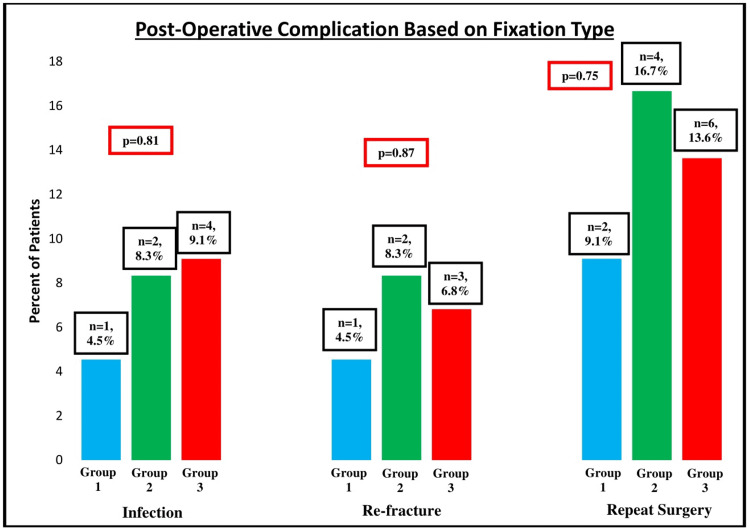
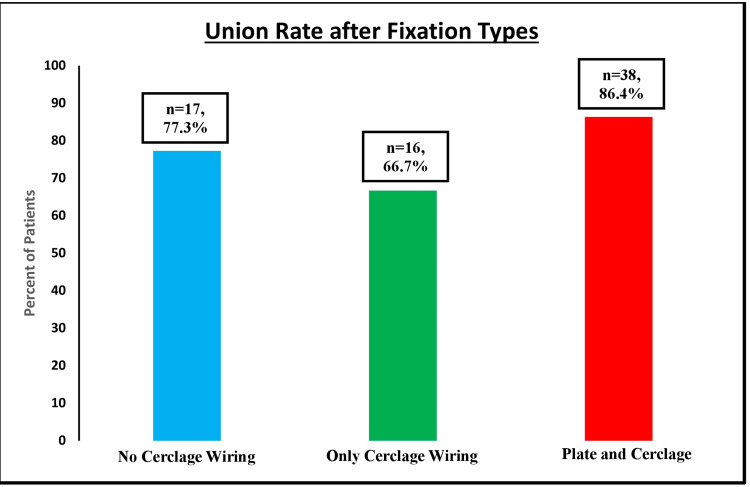
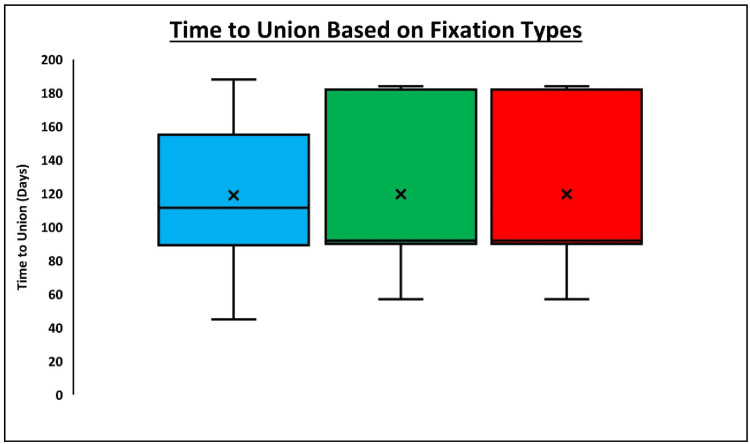
A majority of our patients were females (65.9%) and were older than 71 years of age (65.6%) without diabetes (63.3%) or smoking history (92.2%). Sixty-nine patients progressed to fracture union (76.7%), two (2.2%) to delayed union, and 19 (21.1%) to nonunion. There was no difference in the union rate (p = 0.98) or time to union (p = 0.91) between the fixation methods. Finally, there was no difference in the infection rate (p = 0.81), re-fracture rate (p = 0.87), or re-operation rate (p = 0.75) between the fixation methods.
Periprosthetic femur fractures are common injuries, most commonly occurring after low-energy mechanisms in the elderly female population. While the Vancouver fracture pattern helps to guide the surgical construct used for fixation, the use of cerclage wires does not impact bony union in these injuries. Interestingly, increasing age and female gender were associated with increased union rates. Surgeons should individually consider each patient's demographic as well as fracture type when deciding which construct will achieve stable fixation that allows for fracture healing.
虽然有生物力学和临床研究详细说明了在特定骨折(温哥华B1型和C型)中,环扎钢丝固定与钢板固定相比的等效性,有时甚至是优越性,但尚无研究详细说明所有温哥华B型骨折类型中环扎钢丝固定后的结果。本研究探讨了采用环扎钢丝固定的温哥华B型骨折与未采用该方法固定的骨折在临床结果上是否存在差异。
这项回顾性多中心研究回顾了2007年至2018年期间295例股骨假体周围骨折患者。确定了采用环扎钢丝固定的温哥华B型假体周围骨折,并与未采用环扎钢丝固定的骨折进行比较,其中B1型骨折占33%,B2型骨折占48.4%,B3型骨折占18.6%。记录了每位患者的人口统计学资料、损伤细节、骨折分类、手术细节、骨折愈合情况和术后并发症。
我们的大多数患者为女性(65.9%),年龄超过71岁(65.6%),无糖尿病(63.3%)或吸烟史(92.2%)。69例患者骨折愈合(76.7%),2例(2.2%)延迟愈合,19例(21.1%)未愈合。两种固定方法在愈合率(p = 0.98)或愈合时间(p = 0.91)上没有差异。最后,两种固定方法在感染率(p = 0.81)、再骨折率(p = 0.87)或再次手术率(p = 0.75)上没有差异。
股骨假体周围骨折是常见损伤,最常发生于老年女性人群的低能量损伤机制之后。虽然温哥华骨折分型有助于指导用于固定的手术结构,但使用环扎钢丝对这些损伤的骨愈合没有影响。有趣的是,年龄增长和女性性别与愈合率增加有关。在决定哪种结构能实现稳定固定以促进骨折愈合时,外科医生应分别考虑每位患者的人口统计学资料以及骨折类型。