Miura Kouichi, Maeda Hiroshi, Morimoto Naoki, Watanabe Shunji, Tsukui Mamiko, Takaoka Yoshinari, Nomoto Hiroaki, Goka Rie, Kotani Kazuhiko, Yamamoto Hironori
Department of Medicine, Division of Gastroenterology, Jichi Medical University School of Medicine, 3311-1 Yakushiji, Shimotsuke 329-0498, Tochigi, Japan.
Division of Community and Family Medicine, Center for Community Medicine, Jichi Medical University, 3311-1 Yakushiji, Shimotsuke 329-0498, Japan.
World J Gastrointest Pathophysiol. 2022 May 22;13(3):96-106. doi: 10.4291/wjgp.v13.i3.96.
Vibration-controlled transient elastography (VCTE) is proposed as a second step of examination to assess liver fibrosis in patients with nonalcoholic fatty liver disease (NAFLD) after triaging by the fibrosis-4 (FIB-4) index. Recently, VCTE-based scoring systems, including FibroScan-AST (FAST), Agile 3+, and Agile 4, emerged to determine the status of NAFLD. However, the significance of these scoring systems remains unknown in narrowing the high-risk group of NAFLD patients with comorbidities, including hepatocellular carcinoma (HCC) and esophagogastric varices (EGV).
To clarify the significance of VCTE-based scoring systems to narrow the high-risk group of NAFLD patients with comorbidities.
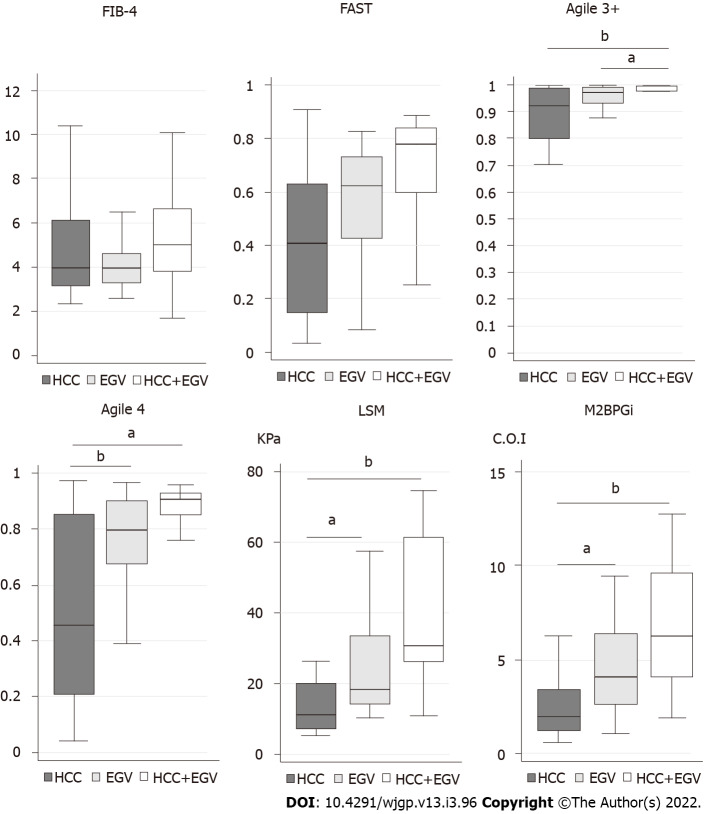
We performed a cross-sectional study to investigate the usefulness of VCTE-based scoring systems and other fibrosis markers to narrow the high-risk group of patients with NAFLD. FIB-4 index was used for the first triage. Risk groups of FAST, Agile 3+, and Agile 4 were stratified according to the published data. Among the 191 patients with NAFLD, there were 26 (14%) and 25 patients (13%) with HCC and EGV, respectively.
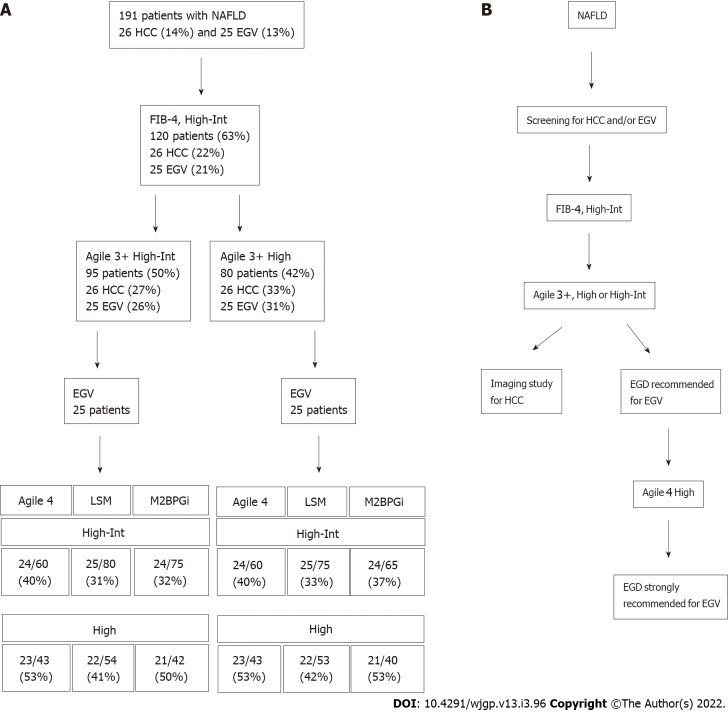
When 1.3 was used as a cutoff value, the FIB-4 index narrowed the risk group to 120 patients, in which all patients with HCC and/or EGV were included. High risk group of Agile 3+ could subsequently narrow the risk group. The prevalence of HCC and EGV at this step were 33% (26/80) and 31% (25/80), respectively. In further narrowing of EGV, Agile 4 aggregated the patients with EGV into 43 patients, of whom 23 (53%) had EGV. FAST failed to narrow the risk group of patients with comorbidities. When 2.6 was used as a cutoff value of the FIB-4 index, three patients with HCC and two patients with EGV were missed at the first triage.
Agile 3+ and Agile 4 are useful to narrow the NAFLD patient group, in which patients may have HCC and/or EGV.
振动控制瞬时弹性成像(VCTE)被提议作为在通过纤维化-4(FIB-4)指数进行分流后评估非酒精性脂肪性肝病(NAFLD)患者肝纤维化的第二步检查。最近,基于VCTE的评分系统,包括FibroScan-AST(FAST)、Agile 3+和Agile 4,应运而生以确定NAFLD的状态。然而,这些评分系统在缩小合并症(包括肝细胞癌(HCC)和食管胃静脉曲张(EGV))的NAFLD高危患者群体方面的意义仍不明确。
阐明基于VCTE的评分系统在缩小合并症NAFLD高危患者群体方面的意义。
我们进行了一项横断面研究,以调查基于VCTE的评分系统和其他纤维化标志物在缩小NAFLD高危患者群体方面的有用性。FIB-4指数用于首次分流。根据已发表的数据对FAST、Agile 3+和Agile 4的风险组进行分层。在191例NAFLD患者中,分别有26例(14%)和25例(13%)患有HCC和EGV。
当以1.3作为截断值时,FIB-4指数将风险组缩小至120例患者,其中包括所有患有HCC和/或EGV的患者。Agile 3+的高危组随后可进一步缩小风险组。此时HCC和EGV的患病率分别为33%(26/80)和31%(25/80)。在进一步缩小EGV风险组时,Agile 4将患有EGV的患者汇总为43例,其中23例(53%)患有EGV。FAST未能缩小合并症患者的风险组。当以2.6作为FIB-4指数的截断值时,首次分流时遗漏了3例HCC患者和2例EGV患者。
Agile 3+和Agile 4有助于缩小可能患有HCC和/或EGV的NAFLD患者群体。