Jin Chongying, Torii Ryo, Ramasamy Anantharaman, Tufaro Vincenzo, Little Callum D, Konstantinou Klio, Tan Yi Ying, Yap Nathan A L, Cooper Jackie, Crake Tom, O'Mahony Constantinos, Rakhit Roby, Egred Mohaned, Ahmed Javed, Karamasis Grigoris, Räber Lorenz, Baumbach Andreas, Mathur Anthony, Bourantas Christos V
Department of Cardiology, Barts Heart Centre, Barts Health NHS Trust, London, United Kingdom.
Department of Cardiology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
Front Cardiovasc Med. 2022 May 26;9:890799. doi: 10.3389/fcvm.2022.890799. eCollection 2022.
Intravascular imaging has been used to assess the morphology of lesions causing an acute coronary syndrome (ACS) in native vessels (NV) and identify differences between plaques that ruptured (PR) and caused an event and those that ruptured without clinical manifestations. However, there is no data about the morphological and physiological characteristics of neoatherosclerotic plaques that ruptured (PR-NA) which constitute a common cause of stent failure.
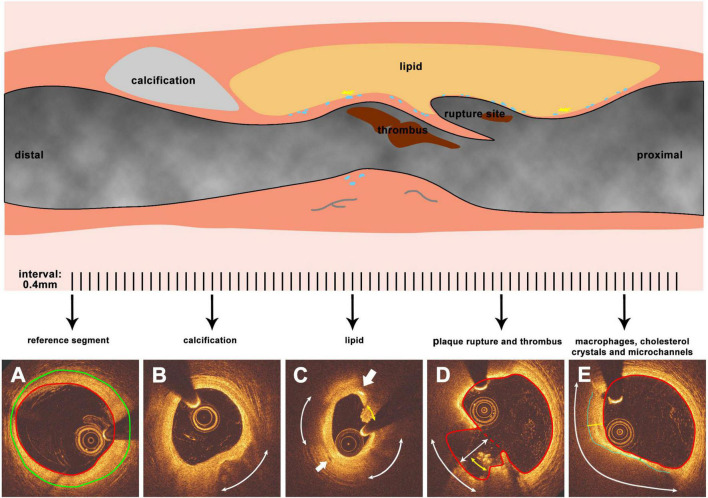
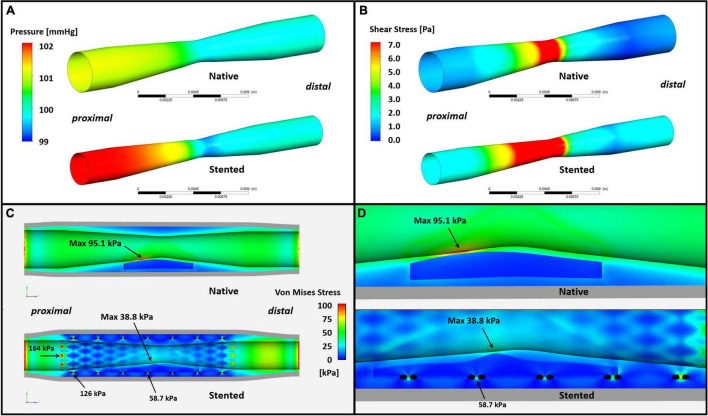
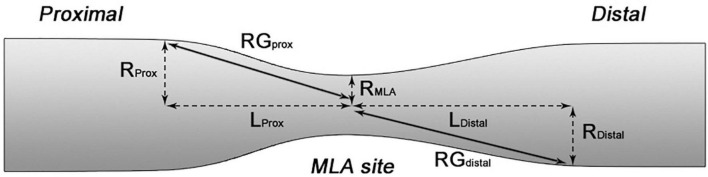
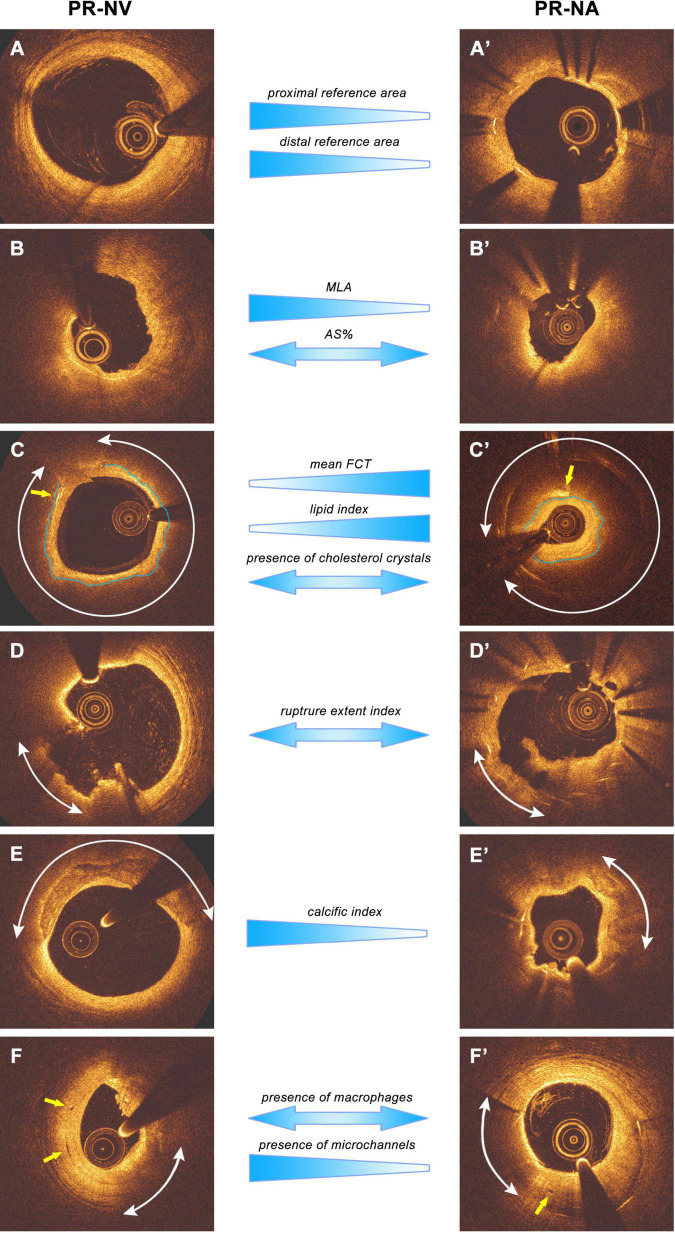
We retrospectively analyzed data from patients admitted with an acute myocardial infarction that had optical coherence tomography (OCT) imaging of the culprit vessel before balloon pre-dilation. OCT pullbacks showing PR were segmented at every 0.4 mm. The extent of the formed cavity, lipid and calcific tissue, thrombus, and macrophages were measured, and the fibrous cap thickness (FCT) and the incidence of micro-channels and cholesterol crystals were reported. These data were used to reconstruct a representative model of the native and neoatherosclerotic lesion geometry that was processed with computational fluid dynamics (CFD) techniques to estimate the distribution of the endothelial shear stress and plaque structural stress.
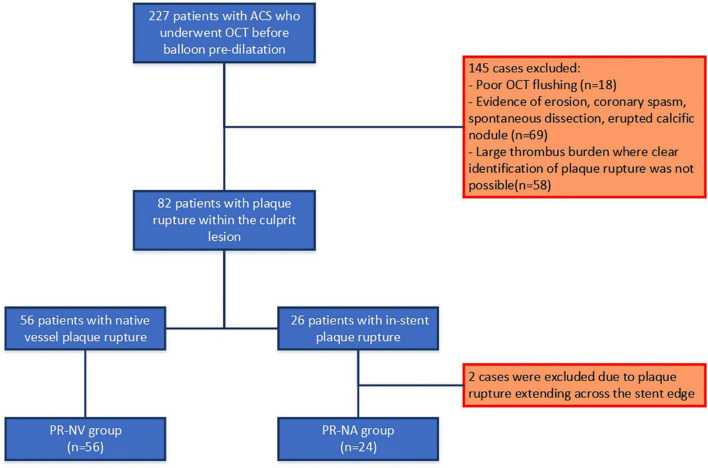
Eighty patients were included in the present analysis: 56 had PR in NV (PR-NV group) and 24 in NA segments (PR-NA group). The PR-NV group had a larger minimum lumen area (2.93 ± 2.03 vs. 2.00 ± 1.26 mm, = 0.015) but similar lesion length and area stenosis compared to PR-NA group. The mean FCT (186 ± 65 vs. 232 ± 80 μm, = 0.009) and the lipid index was smaller (16.7 ± 13.8 vs. 25.9 ± 14.1, = 0.008) while the of calcific index (8.3 ± 9.5 vs. 2.2 ± 1.6%, = 0.002) and the incidence of micro-channels (41.4 vs. 12.5%, = 0.013) was higher in the PR-NV group. Conversely, there was no difference in the incidence of cholesterol crystals, thrombus burden or the location of the rupture site between groups. CFD analysis revealed higher maximum endothelial shear stress (19.1 vs. 11.0 Pa) and lower maximum plaque structural stress (38.8 vs. 95.1 kPa) in the PR-NA compared to the PR-NV model.
We reported significant morphological and physiological differences between culprit ruptured plaques in native and stented segments. Further research is needed to better understand the causes of these differences and the mechanisms regulating neoatherosclerotic lesion destabilization.
血管内成像已被用于评估导致急性冠状动脉综合征(ACS)的天然血管(NV)病变的形态,并识别破裂(PR)并引发事件的斑块与破裂但无临床表现的斑块之间的差异。然而,关于构成支架失败常见原因的新生动脉粥样硬化斑块破裂(PR-NA)的形态和生理特征尚无数据。
我们回顾性分析了因急性心肌梗死入院且在球囊预扩张前对罪犯血管进行光学相干断层扫描(OCT)成像的患者数据。显示PR的OCT回撤图像以每0.4毫米进行分割。测量形成腔、脂质和钙化组织、血栓及巨噬细胞的范围,并报告纤维帽厚度(FCT)、微通道发生率和胆固醇结晶情况。这些数据用于重建天然和新生动脉粥样硬化病变几何结构的代表性模型,并采用计算流体动力学(CFD)技术进行处理,以估计内皮剪切应力和斑块结构应力的分布。
本分析纳入了80例患者:56例在NV中有PR(PR-NV组),24例在新生动脉粥样硬化节段中有PR(PR-NA组)。与PR-NA组相比,PR-NV组的最小管腔面积更大(2.93±2.03对2.00±1.26平方毫米,P=0.015),但病变长度和面积狭窄情况相似。PR-NV组的平均FCT(186±65对232±80微米,P=0.009)和脂质指数更小(16.7±13.8对25.9±14.1,P=0.008),而钙化指数(8.3±9.5对2.2±1.6%,P=0.002)和微通道发生率(41.4对12.5%,P=0.013)更高。相反,两组之间胆固醇结晶发生率、血栓负荷或破裂部位位置无差异。CFD分析显示,与PR-NV模型相比,PR-NA模型的最大内皮剪切应力更高(19.1对11.0帕),最大斑块结构应力更低(38.8对95.1千帕)。
我们报告了天然和支架植入节段中罪犯破裂斑块之间存在显著的形态和生理差异。需要进一步研究以更好地理解这些差异的原因以及调节新生动脉粥样硬化病变不稳定的机制。