Cattaneo Chiara, Marchesi Francesco, Terrenato Irene, Bonuomo Valentina, Fracchiolla Nicola Stefano, Delia Mario, Criscuolo Marianna, Candoni Anna, Prezioso Lucia, Facchinelli Davide, Pasciolla Crescenza, Del Principe Maria Ilaria, Dargenio Michelina, Buquicchio Caterina, Mitra Maria Enza, Farina Francesca, Borlenghi Erika, Nadali Gianpaolo, Gagliardi Vito Pier, Fianchi Luana, Sciumè Mariarita, Menna Pierantonio, Busca Alessandro, Rossi Giuseppe, Pagano Livio
Hematology, Azienda Socio Sanitaria Territoriale-Spedali Civili, 25123 Brescia, Italy.
Hematology and Stem Cell Transplantation Unit, Istituto di Ricovero e Cura a Carattere Scientifico Regina Elena National Cancer Institute, 00144 Roma, Italy.
J Fungi (Basel). 2022 May 29;8(6):583. doi: 10.3390/jof8060583.
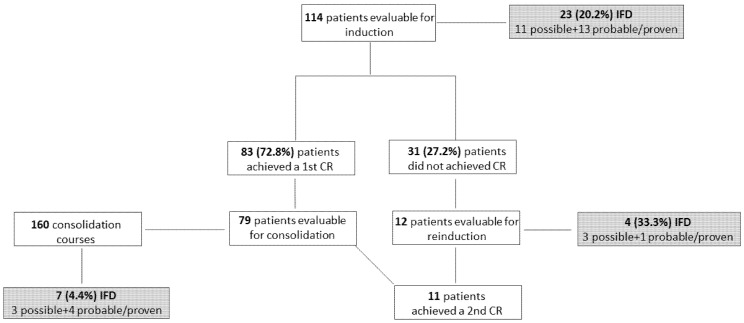
The potential drug-drug interactions of midostaurin may impact the choice of antifungal (AF) prophylaxis in FLT3-positive acute myeloid leukemia (AML) patients. To evaluate the incidence of invasive fungal diseases (IFD) during the treatment of FLT3-mutated AML patients and to correlate it to the different AF prophylaxis strategies, we planned a multicenter observational study involving 15 SEIFEM centers. One hundred fourteen patients treated with chemotherapy + midostaurin as induction/reinduction, consolidation or both were enrolled. During induction, the incidence of probable/proven and possible IFD was 10.5% and 9.7%, respectively; no statistically significant difference was observed according to the different AF strategy adopted. The median duration of neutropenia was similar in patients with or without IFD. Proven/probable and possible IFD incidence was 2.4% and 1.8%, respectively, during consolidation. Age was the only risk factor for IFD (OR, 95% CI, 1.10 [1.03-1.19]) and complete remission achievement after first induction the only one for survival (OR, 95% CI, 5.12 [1.93-13.60]). The rate of midostaurin discontinuation was similar across different AF strategies. The IFD attributable mortality during induction was 8.3%. In conclusion, the 20.2% overall incidence of IFD occurring in FLT3-mutated AML during induction with chemotherapy + midostaurin, regardless of AF strategy type, was noteworthy, and merits further study, particularly in elderly patients.
米哚妥林潜在的药物相互作用可能会影响FLT3阳性急性髓系白血病(AML)患者抗真菌(AF)预防措施的选择。为了评估FLT3突变AML患者治疗期间侵袭性真菌病(IFD)的发生率,并将其与不同的AF预防策略相关联,我们计划开展一项涉及15个SEIFEM中心的多中心观察性研究。纳入了114例接受化疗+米哚妥林进行诱导/再诱导、巩固治疗或两者兼有的患者。诱导治疗期间,确诊/高度疑似和可能的IFD发生率分别为10.5%和9.7%;根据采用的不同AF策略,未观察到统计学上的显著差异。中性粒细胞减少的中位持续时间在有或无IFD的患者中相似。巩固治疗期间,确诊/高度疑似和可能的IFD发生率分别为2.4%和1.8%。年龄是IFD的唯一危险因素(OR,95%CI,1.10[1.03-1.19]),首次诱导后达到完全缓解是生存的唯一危险因素(OR,95%CI,5.12[1.93-13.60])。不同AF策略下米哚妥林停药率相似。诱导治疗期间IFD导致的死亡率为8.3%。总之,在化疗+米哚妥林诱导治疗期间,FLT3突变AML患者中IFD的总体发生率为20.2%,无论AF策略类型如何,这一发生率都值得关注,值得进一步研究,尤其是在老年患者中。