Karakonstantis Stamatis, Rousaki Maria, Kritsotakis Evangelos I
Internal Medicine Department, Infectious Diseases Division, University Hospital of Heraklion, 71500 Heraklion, Greece.
Master of Public Health Program, Department of Social Medicine, School of Medicine, University of Crete, 70013 Heraklion, Greece.
Antibiotics (Basel). 2022 May 27;11(6):723. doi: 10.3390/antibiotics11060723.
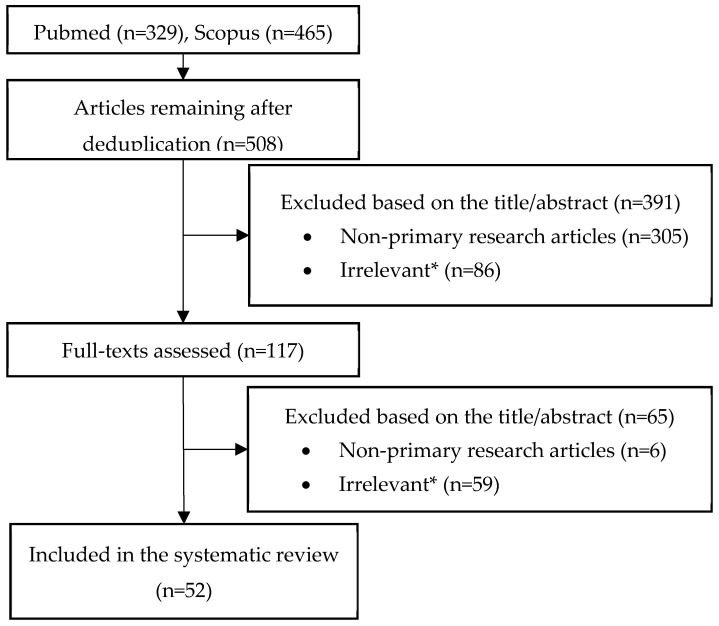
Cefiderocol appears promising, as it can overcome most β-lactam resistance mechanisms (including β-lactamases, porin mutations, and efflux pumps). Resistance is uncommon according to large multinational cohorts, including against isolates resistant to carbapenems, ceftazidime/avibactam, ceftolozane/tazobactam, and colistin. However, alarming proportions of resistance have been reported in some recent cohorts (up to 50%). A systematic review was conducted in PubMed and Scopus from inception to May 2022 to review mechanisms of resistance, prevalence of heteroresistance, and in vivo emergence of resistance to cefiderocol during treatment. A variety of mechanisms, typically acting in concert, have been reported to confer resistance to cefiderocol: β-lactamases (especially NDM, KPC and AmpC variants conferring resistance to ceftazidime/avibactam, OXA-427, and PER- and SHV-type ESBLs), porin mutations, and mutations affecting siderophore receptors, efflux pumps, and target (PBP-3) modifications. Coexpression of multiple β-lactamases, often in combination with permeability defects, appears to be the main mechanism of resistance. Heteroresistance is highly prevalent (especially in ), but its clinical impact is unclear, considering that in vivo emergence of resistance appears to be low in clinical studies. Nevertheless, cases of in vivo emerging cefiderocol resistance are increasingly being reported. Continued surveillance of cefiderocol's activity is important as this agent is introduced in clinical practice.
头孢地尔似乎很有前景,因为它可以克服大多数β-内酰胺耐药机制(包括β-内酰胺酶、孔蛋白突变和外排泵)。根据大型跨国队列研究,耐药情况并不常见,包括对碳青霉烯类、头孢他啶/阿维巴坦、头孢洛扎/他唑巴坦和黏菌素耐药的菌株。然而,最近一些队列研究报告了令人担忧的耐药比例(高达50%)。我们在PubMed和Scopus数据库中进行了一项系统综述,涵盖从数据库建立至2022年5月的文献,以回顾头孢地尔的耐药机制、异质性耐药的发生率以及治疗期间体内耐药的出现情况。据报道,多种机制通常协同作用,可导致对头孢地尔产生耐药:β-内酰胺酶(尤其是对头孢他啶/阿维巴坦耐药的NDM、KPC和AmpC变体、OXA-427以及PER型和SHV型超广谱β-内酰胺酶)、孔蛋白突变以及影响铁载体受体、外排泵和靶点(PBP-3)修饰的突变。多种β-内酰胺酶的共表达,通常与通透性缺陷共同作用,似乎是主要的耐药机制。异质性耐药非常普遍(尤其是在……),但其临床影响尚不清楚,因为在临床研究中体内耐药的出现似乎较少。尽管如此,越来越多关于体内出现头孢地尔耐药的病例报告。随着这种药物在临床实践中的应用,持续监测头孢地尔的活性很重要。