Moroder Philipp, Lacheta Lucca, Minkus Marvin, Karpinski Katrin, Uhing Frank, De Souza Sheldon, van der Merwe Michael, Akgün Doruk
Schulthess Clinic, 8008 Zürich, Switzerland.
Arthrex GMBH, D-81249 Munich, Germany.
J Clin Med. 2022 Jun 10;11(12):3324. doi: 10.3390/jcm11123324.
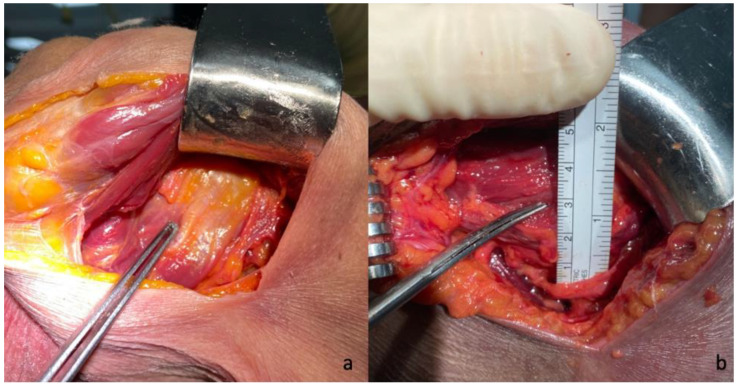
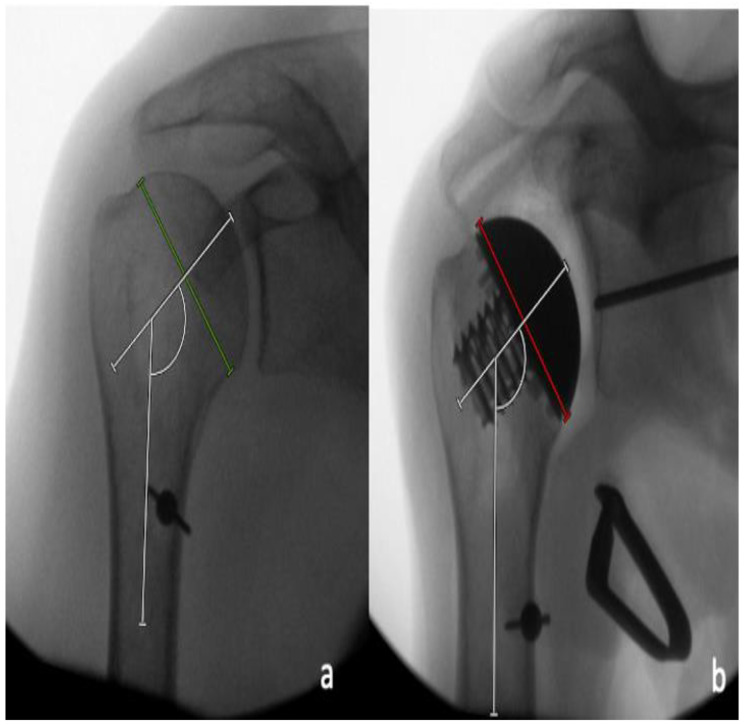
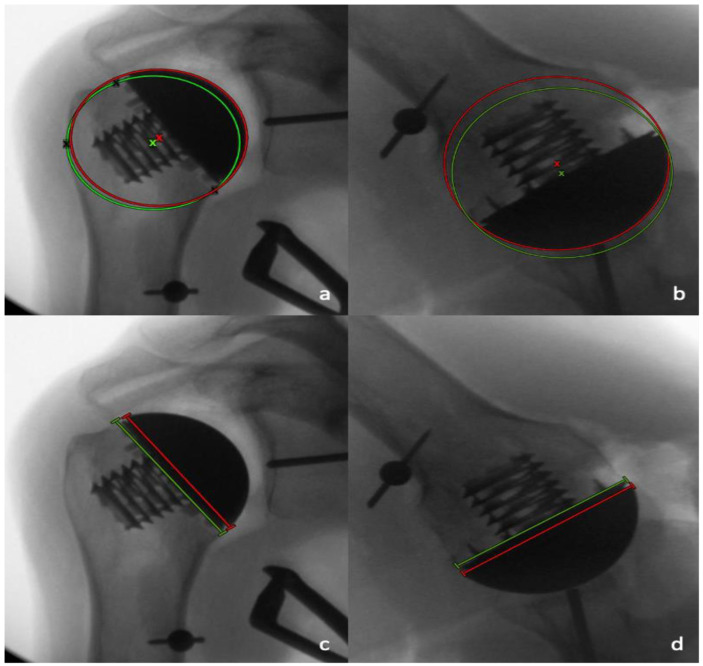
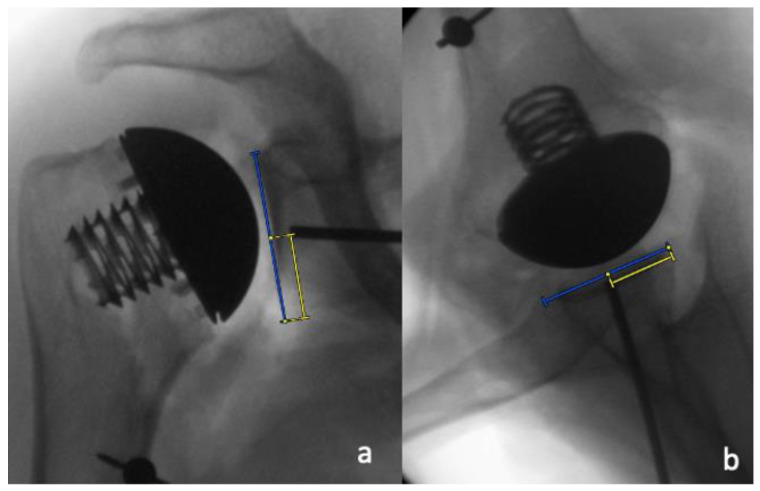
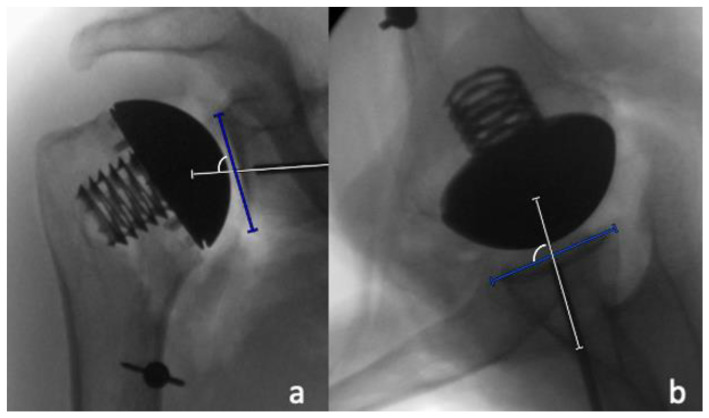
The goal of this study was to compare the effectiveness of a rotator cuff-sparing postero-inferior (PI) approach with subdeltoidal access to the traditional subscapularis-takedown deltopectoral approach, in terms of implant sizing and positioning in anatomical total shoulder arthroplasty (aTSA). This study involved 18 human cadaveric shoulders with intact rotator cuffs and no evidence of head deforming osteoarthritis. An Eclipse stemless aTSA (Arthrex, Naples, FL, USA) was implanted in nine randomly selected specimens using a standard subscapularis-tenotomy deltopectoral approach, and in the other nine specimens using the cuff-sparing PI approach. Pre- and postoperative antero-posterior (AP) and axillary fluoroscopic radiographs were analyzed by two independent, blinded raters for the following parameters: (1) anatomic and prosthetic neck-shaft angle (NSA); (2) the shift between the anatomic and prosthetic center of rotation (COR); (3) anatomical size matching of the prosthetic humeral head; (4) the calculated Anatomic Reconstruction Score (ARS); (5) glenoid positioning; as well as (6) glenoid inclination and version. While the COR was slightly but significantly positioned ( = 0.031) to be more medial in the PI approach group (3.7 ± 3.4%, range: -2.3% to 8.7%) than in the deltopectoral approach group (-0.2 ± 3.6%, range: -6.9% to 4.1%), on average, none of the remaining measured radiographic parameters significantly differed between both groups (PI approach group vs. deltopectoral group: NSA 130° vs. 127°, = 0.57; COR supero-inferior, 2.6% vs. 1.0%, = 0.35; COR antero-posterior, 0.9% vs. 1.7%, = 0.57; head size supero-inferior, 97.3% vs. 98.5%, = 0.15; head size antero-posterior, 101.1% vs. 100.6%, = 0.54; ARS, 8.4 vs. 9.3, = 0.13; glenoid positioning supero-inferior, 49.1% vs. 51.1%, = 0.33; glenoid positioning antero-posterior, 49.3% vs. 50.4%, = 0.23; glenoid inclination, 86° vs. 88°, = 0.27; and glenoid retroversion, 91° vs. 89°, = 0.27). A PI approach allows for sufficient exposure and orientation to perform rotator-cuff sparing aTSA with acceptable implant sizing and positioning in cadaveric specimens.
本研究的目的是,在解剖型全肩关节置换术(aTSA)中,就植入物的尺寸选择和定位而言,比较保留肩袖的后下(PI)入路与经三角肌下入路至传统肩胛下肌切断胸大肌三角肌入路的有效性。本研究纳入了18个肩袖完整且无肱骨头变形性骨关节炎证据的人体尸体肩关节。使用标准的肩胛下肌切断胸大肌三角肌入路,将Eclipse无柄aTSA(美国佛罗里达州那不勒斯市的Arthrex公司)植入9个随机选择的标本中,在另外9个标本中使用保留肩袖的PI入路。由两名独立的、不知情的评估者分析术前和术后的前后位(AP)和腋位透视X线片,以评估以下参数:(1)解剖学和假体的颈干角(NSA);(2)解剖学和假体旋转中心(COR)之间的偏移;(3)假体肱骨头的解剖学尺寸匹配;(4)计算得出的解剖重建评分(ARS);(5)关节盂定位;以及(6)关节盂倾斜度和版本。虽然PI入路组的COR平均略微但显著地( = 0.031)比胸大肌三角肌入路组更偏向内侧(PI入路组为3.7 ± 3.4%,范围:-2.3%至8.7%;胸大肌三角肌入路组为-0.2 ± 3.6%,范围:-6.9%至4.1%),但两组之间其余测量的影像学参数均无显著差异(PI入路组与胸大肌三角肌入路组:NSA分别为130°和127°, = 0.57;COR上下方向分别为2.6%和1.0%, = 0.35;COR前后方向分别为0.9%和1.7%, = 0.57;肱骨头尺寸上下方向分别为97.3%和98.5%, = 0.15;肱骨头尺寸前后方向分别为101.1%和100.6%, = 0.54;ARS分别为8.4和9.3, = 0.13;关节盂定位上下方向分别为49.1%和51.1%, = 0.33;关节盂定位前后方向分别为49.3%和50.4%, = 0.23;关节盂倾斜度分别为86°和88°, = 0.27;关节盂后倾分别为91°和89°, = 0.27)。PI入路能够提供足够的暴露和定位,以便在尸体标本中进行保留肩袖的aTSA,并获得可接受的植入物尺寸选择和定位。