Yale University School of Medicine, New Haven, Connecticut, USA.
Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Transfusion. 2022 Jul;62(7):1365-1376. doi: 10.1111/trf.16987. Epub 2022 Jun 24.
Platelet transfusion carries risk of transfusion-transmitted infection (TTI). Pathogen reduction of platelet components (PRPC) is designed to reduce TTI. Pulmonary adverse events (AEs), including transfusion-related acute lung injury and acute respiratory distress syndrome (ARDS) occur with platelet transfusion.
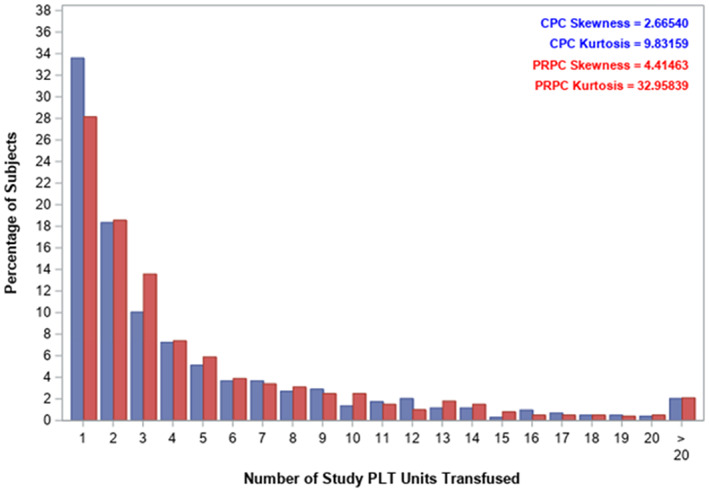
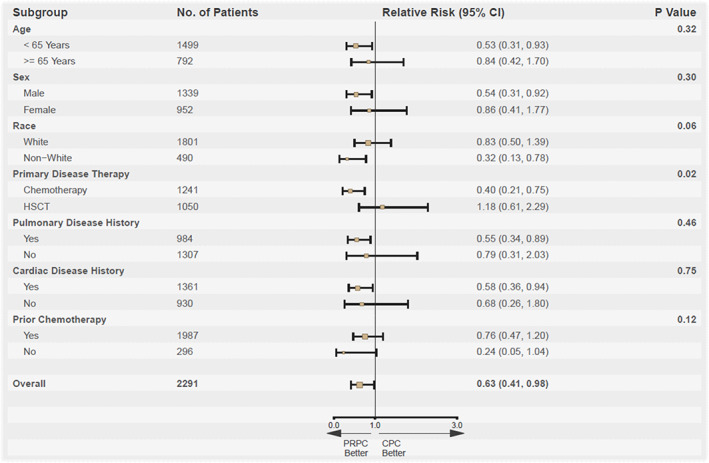
An open label, sequential cohort study of transfusion-dependent hematology-oncology patients was conducted to compare pulmonary safety of PRPC with conventional PC (CPC). The primary outcome was the incidence of treatment-emergent assisted mechanical ventilation (TEAMV) by non-inferiority. Secondary outcomes included: time to TEAMV, ARDS, pulmonary AEs, peri-transfusion AE, hemorrhagic AE, transfusion reactions (TRs), PC and red blood cell (RBC) use, and mortality.
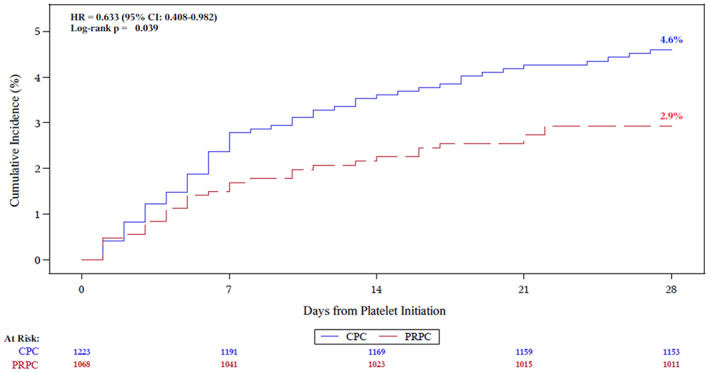
By modified intent-to-treat (mITT), 1068 patients received 5277 PRPC and 1223 patients received 5487 CPC. The cohorts had similar demographics, primary disease, and primary therapy. PRPC were non-inferior to CPC for TEAMV (treatment difference -1.7%, 95% CI: (-3.3% to -0.1%); odds ratio = 0.53, 95% CI: (0.30, 0.94). The cumulative incidence of TEAMV for PRPC (2.9%) was significantly less than CPC (4.6%, p = .039). The incidence of ARDS was less, but not significantly different, for PRPC (1.0% vs. 1.8%, p = .151; odds ratio = 0.57, 95% CI: (0.27, 1.18). AE, pulmonary AE, and mortality were not different between cohorts. TRs were similar for PRPC and CPC (8.3% vs. 9.7%, p = .256); and allergic TR were significantly less with PRPC (p = .006). PC and RBC use were not increased with PRPC.
PRPC demonstrated reduced TEAMV with no excess treatment-related pulmonary morbidity.
血小板输注存在输血传播感染(TTI)的风险。血小板成分病原体减少(PRPC)旨在降低 TTI。血小板输注会引起肺部不良事件(AE),包括输血相关急性肺损伤和急性呼吸窘迫综合征(ARDS)。
对依赖输血的血液肿瘤患者进行了一项开放标签、连续队列研究,以比较 PRPC 与常规血小板(CPC)的肺部安全性。主要结局为非劣效性治疗后出现的有创机械通气(TEAMV)发生率。次要结局包括:TEAMV 时间、ARDS、肺部 AE、输血前 AE、出血性 AE、输血反应(TR)、血小板和红细胞(RBC)使用以及死亡率。
根据改良意向治疗(mITT),1068 例患者接受了 5277 次 PRPC 输注,1223 例患者接受了 5487 次 CPC 输注。两组患者的人口统计学特征、主要疾病和主要治疗方法相似。PRPC 与 CPC 相比,TEAMV 无差异(治疗差异-1.7%,95%CI:(-3.3%至-0.1%);优势比=0.53,95%CI:(0.30,0.94)。PRPC 的 TEAMV 累积发生率(2.9%)明显低于 CPC(4.6%,p=0.039)。PRPC 的 ARDS 发生率虽较低,但无统计学差异(1.0% vs. 1.8%,p=0.151;优势比=0.57,95%CI:(0.27,1.18)。两组患者的 AE、肺部 AE 和死亡率无差异。PRPC 和 CPC 的 TR 相似(8.3% vs. 9.7%,p=0.256);且 PRPC 的过敏 TR 明显减少(p=0.006)。PRPC 并未增加血小板和 RBC 的使用。
PRPC 降低了 TEAMV,且未增加与治疗相关的肺部发病率。