Drexel University College of Medicine, Philadelphia, PA, USA.
AbbVie Inc., North Chicago, IL, USA.
Arthritis Res Ther. 2022 Jun 24;24(1):155. doi: 10.1186/s13075-022-02813-x.
In previous clinical trials, patients with active rheumatoid arthritis (RA) treated with upadacitinib (UPA) have improved patient-reported outcomes (PROs). This post hoc analysis of SELECT-CHOICE, a phase 3 clinical trial, evaluated the impact of UPA vs abatacept (ABA) with background conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) on PROs in patients with RA with inadequate response or intolerance to biologic disease-modifying antirheumatic drugs (bDMARD-IR).
Patients in SELECT-CHOICE received UPA (oral 15 mg/day) or ABA (intravenous). PROs evaluated included Patient Global Assessment of Disease Activity (PtGA) by visual analog scale (VAS), patient's assessment of pain by VAS, Health Assessment Questionnaire Disability Index (HAQ-DI), morning stiffness duration and severity, 36-Item Short Form Health Survey (SF-36), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), Work Productivity and Activity Impairment (WPAI), and EQ-5D 5-Level (EQ-5D-5L) index score. Least squares mean (LSM) changes from baseline to weeks 12 and 24 were based on an analysis of covariance model. Proportions of patients reporting improvements ≥ minimal clinically important differences (MCID) were compared using chi-square tests.
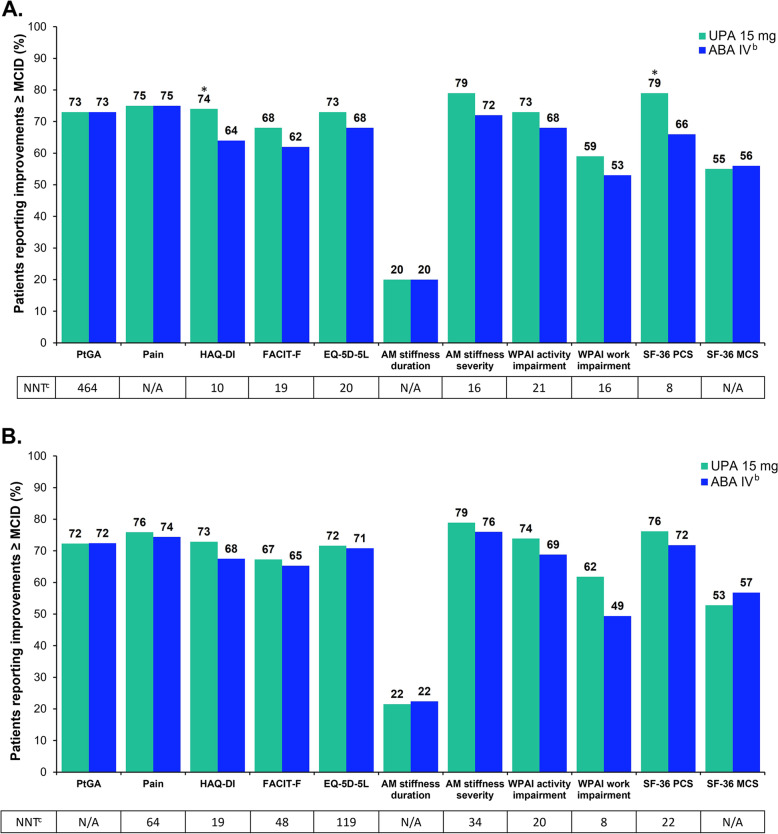
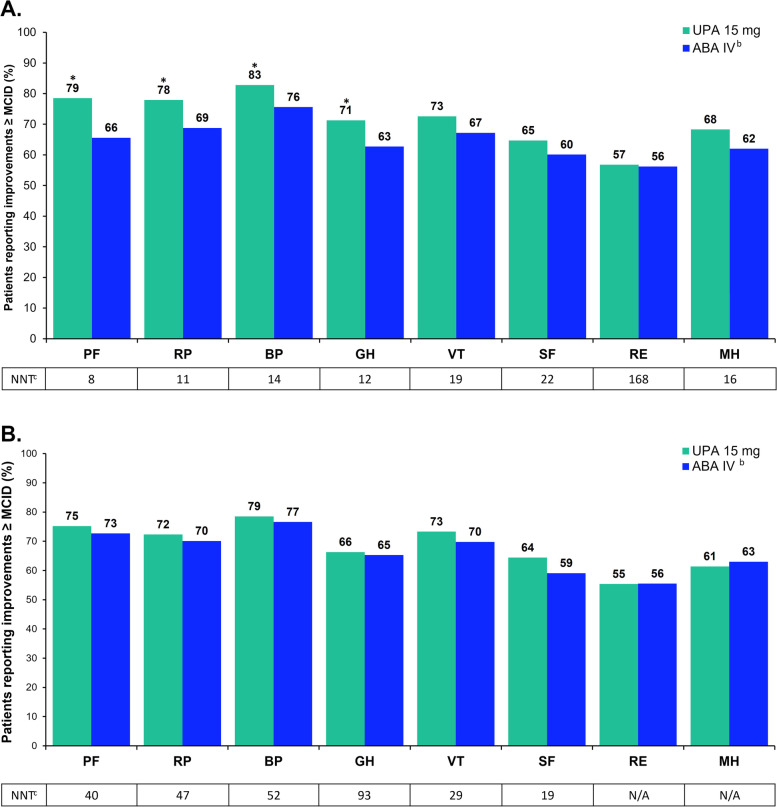
Data from 612 patients were analyzed (UPA, n=303; ABA, n=309). Mean age was 56 years and mean disease duration was 12 years. One-third received ≥2 prior bDMARDs and 72% received concomitant methotrexate at baseline. At week 12, UPA- vs ABA-treated patients had significantly greater improvements in PtGA, pain, HAQ-DI, morning stiffness severity, EQ-5D-5L, 2/4 WPAI domains, and 3/8 SF-36 domains and Physical Component Summary (PCS) scores (P<0.05); significant differences persisted at week 24 for HAQ-DI, morning stiffness severity, SF-36 PCS and bodily pain domain, and WPAI activity impairment domain. At week 12, significantly more UPA- vs ABA-treated patients reported improvements ≥MCID in HAQ-DI (74% vs 64%) and SF-36 PCS (79% vs 66%) and 4/8 domain scores (P<0.05).
At week 12, UPA vs ABA treatment elicited greater improvements in key domains of physical functioning, pain, and general health and earlier improvements in HAQ-DI. Overall, more UPA- vs ABA-treated patients achieved ≥MCID in most PROs at all timepoints; however, not all differences were statistically significant. These data, however, highlight the faster response to UPA treatment.
NCT03086343 , March 22, 2017.
在之前的临床试验中,接受乌帕替尼(UPA)治疗的活动性类风湿关节炎(RA)患者的患者报告结局(PRO)得到了改善。这项来自 3 期临床试验 SELECT-CHOICE 的事后分析评估了与阿巴西普(ABA)相比,UPA 联合背景下常规合成改善病情抗风湿药(csDMARDs)治疗对生物改善病情抗风湿药(bDMARD)反应不足或不耐受(bDMARD-IR)的 RA 患者 PRO 的影响。
SELECT-CHOICE 中的患者接受 UPA(口服 15mg/天)或 ABA(静脉注射)治疗。评估的 PRO 包括患者整体疾病活动度评估(PtGA)的视觉模拟量表(VAS)评分、患者疼痛的评估 VAS 评分、健康评估问卷残疾指数(HAQ-DI)、晨僵时间和严重程度、36 项简明健康调查(SF-36)、慢性疾病治疗疲劳功能性评估(FACIT-F)、工作生产力和活动障碍(WPAI)以及 EQ-5D 5 级(EQ-5D-5L)指数评分。基于协方差分析模型,从基线到第 12 周和第 24 周的最小二乘均值(LSM)变化。使用卡方检验比较报告改善≥最小临床重要差异(MCID)的患者比例。
共分析了 612 名患者的数据(UPA 组,n=303;ABA 组,n=309)。平均年龄为 56 岁,平均病程为 12 年。三分之一的患者接受了≥2 种先前的 bDMARD,72%的患者在基线时接受了甲氨蝶呤。在第 12 周,与 ABA 治疗相比,UPA 治疗的患者在 PtGA、疼痛、HAQ-DI、晨僵严重程度、EQ-5D-5L、2/4 WPAI 域和 3/8 SF-36 域以及生理成分综合评分(PCS)上有显著改善(P<0.05);在第 24 周时,HAQ-DI、晨僵严重程度、SF-36 PCS 和身体疼痛域以及 WPAI 活动障碍域的差异仍持续存在。在第 12 周,与 ABA 治疗相比,更多的 UPA 治疗的患者在 HAQ-DI(74% vs 64%)和 SF-36 PCS(79% vs 66%)以及 4/8 个域评分上报告了≥MCID 的改善(P<0.05)。
在第 12 周时,与 ABA 治疗相比,UPA 治疗在物理功能、疼痛和总体健康的关键领域引起了更大的改善,并且在 HAQ-DI 方面更早出现改善。总体而言,在所有时间点,与接受 ABA 治疗的患者相比,更多的 UPA 治疗的患者在大多数 PRO 中达到了≥MCID;然而,并非所有差异均具有统计学意义。然而,这些数据突出了 UPA 治疗的更快反应。
NCT03086343,2017 年 3 月 22 日。