Chu Stanley, Kilinc Ozden, Pradella Maurice, Weiss Elizabeth, Baraboo Justin, Maroun Anthony, Jarvis Kelly, Mehta Christopher K, Malaisrie S Chris, Hoel Andrew W, Carr James C, Markl Michael, Allen Bradley D
Department of Radiology, Northwestern University, Chicago, IL, United States.
Department of Biomedical Engineering, Northwestern University, Chicago, IL, United States.
Front Cardiovasc Med. 2022 Jun 9;9:905718. doi: 10.3389/fcvm.2022.905718. eCollection 2022.
The purpose of our study was to assess the value of true lumen and false lumen hemodynamics compared to aortic morphological measurements for predicting adverse-aorta related outcomes (AARO) and aortic growth in patients with type B aortic dissection (TBAD).
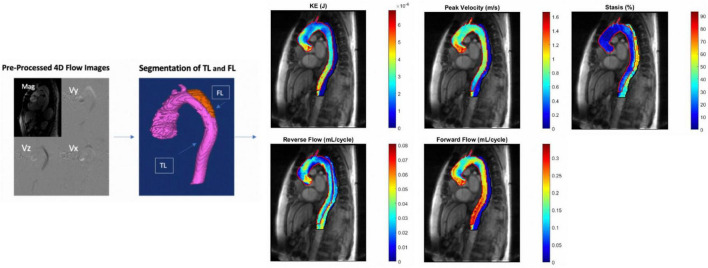
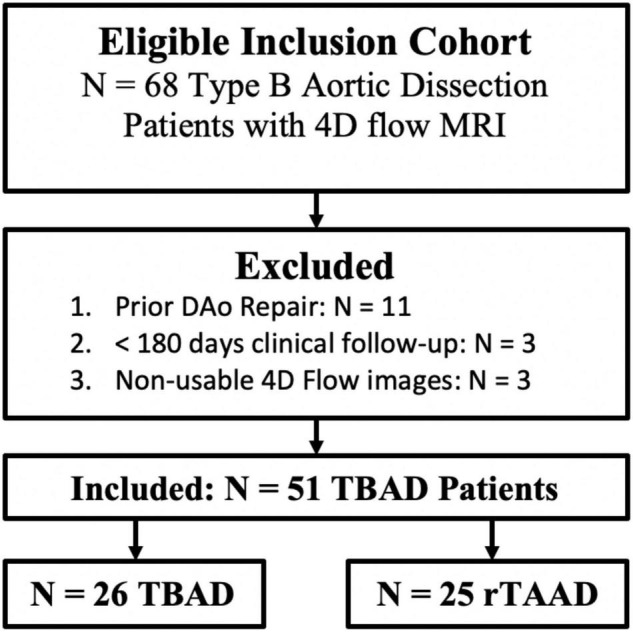
Using an IRB approved protocol, we retrospectively identified patients with descending aorta (DAo) dissection at a large tertiary center. Inclusion criteria includes known TBAD with ≥ 6 months of clinical follow-up after initial presentation for TBAD or after ascending aorta intervention for patients with repaired type A dissection with residual type B aortic dissection (rTAAD). Patients with prior descending aorta intervention were excluded. The FL and TL of each patient were manually segmented from 4D flow MRI data, and 3D parametric maps of aortic hemodynamics were generated. Groups were divided based on (1) presence vs. absence of AARO and (2) growth rate ≥ vs. < 3 mm/year. True and false lumen kinetic energy (KE), stasis, peak velocity (PV), reverse/forward flow (RF/FF), FL to TL KE ratio, as well as index aortic diameter were compared between groups using the Mann-Whitney or independent -test.
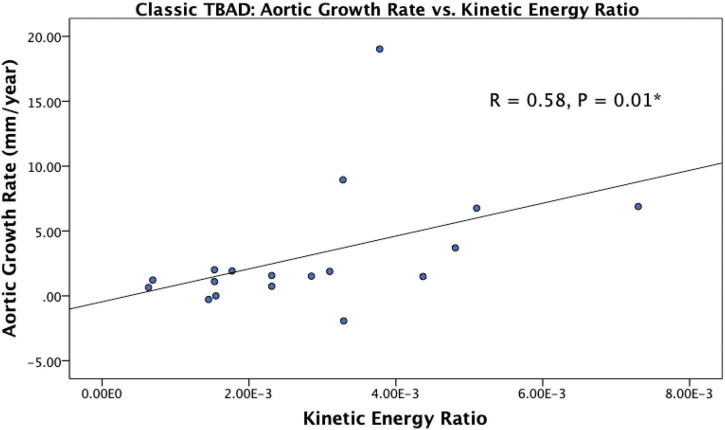
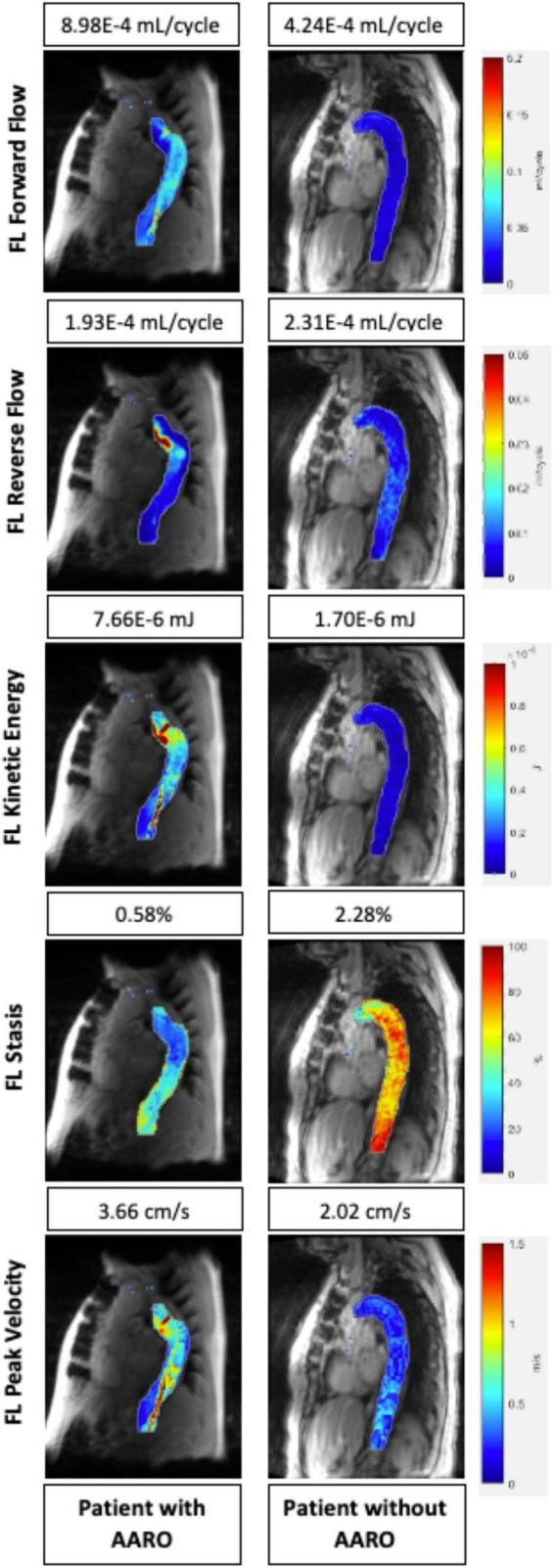
A total of = 51 patients (age: 58.4 ± 15.0 years, M/F: 31/20) were included for analysis of AARO. This group contained = 26 patients with TBAD and = 25 patients with rTAAD. In the overall cohort, AARO patients had larger baseline diameters, lower FL-RF, FL stasis, TL-KE, TL-FF and TL-PV. Among patients with TBAD, those with AAROs had larger baseline diameter, lower FL stasis and TL-PV. In both the overall cohort and in the subgroup of TBAD, subjects with aortic growth ≥ 3mm/year, patients had a higher KE ratio.
Our study suggests that 4D flow MRI is a promising tool for TBAD evaluation that can provide information beyond traditional MRA or CTA. 4D flow has the potential to become an integral aspect of TBAD work-up, as hemodynamic assessment may allow earlier identification of at-risk patients who could benefit from earlier intervention.
我们研究的目的是评估与主动脉形态测量相比,真腔和假腔血流动力学对于预测B型主动脉夹层(TBAD)患者不良主动脉相关结局(AARO)和主动脉生长的价值。
使用经机构审查委员会批准的方案,我们在一家大型三级中心回顾性地识别降主动脉(DAo)夹层患者。纳入标准包括初次出现TBAD后或A型夹层修复且残留B型主动脉夹层(rTAAD)的患者进行升主动脉干预后有≥6个月临床随访的已知TBAD。排除先前有降主动脉干预的患者。从4D流动磁共振成像(MRI)数据中手动分割出每位患者的假腔(FL)和真腔(TL),并生成主动脉血流动力学的3D参数图。根据(1)是否存在AARO和(2)生长速率≥与<3毫米/年进行分组。使用Mann-Whitney检验或独立t检验比较组间真腔和假腔的动能(KE)、血流淤滞、峰值速度(PV)、反向/正向血流(RF/FF)、FL与TL的KE比值以及主动脉直径指数。
共有51例患者(年龄:58.4±15.0岁,男/女:31/20)纳入AARO分析。该组包括26例TBAD患者和25例rTAAD患者。在整个队列中,发生AARO的患者基线直径更大,FL-RF、FL血流淤滞、TL-KE、TL-FF和TL-PV更低。在TBAD患者中,发生AARO的患者基线直径更大,FL血流淤滞和TL-PV更低。在整个队列和TBAD亚组中,主动脉生长≥3毫米/年的患者KE比值更高。
我们的研究表明,4D流动MRI是一种有前景的TBAD评估工具,可提供超越传统磁共振血管造影(MRA)或计算机断层血管造影(CTA)的信息。4D流动有潜力成为TBAD检查的一个组成部分,因为血流动力学评估可能允许更早识别可从早期干预中获益的高危患者。