Servicio de Pediatria. Hospital Universitario 12 de Octubre, Servicio Madrileño de Salud (SERMAS), Madrid, Spain.
Unidad Pediátrica de Investigación y Ensayos Clínicos (UPIC). Instituto de Investigación Sanitaria Hospital 12 de Octubre (i+12), Fundación Biomedica del Hospital Universitario 12 de Octubre (FIB-H12O), Madrid, Spain.
Trials. 2022 Jun 27;23(1):531. doi: 10.1186/s13063-022-06203-1.
Pneumonia is the primary cause of death among HIV-infected children in Africa, with mortality rates as high as 35-40% in infants hospitalized with severe pneumonia. Bacterial pathogens and Pneumocystis jirovecii are well known causes of pneumonia-related death, but other important causes such as cytomegalovirus (CMV) and tuberculosis (TB) remain under-recognized and undertreated. The immune response elicited by CMV may be associated with the risk of developing TB and TB disease progression, and CMV may accelerate disease caused both by HIV and TB. Minimally invasive autopsies confirm that CMV and TB are unrecognized causes of death in children with HIV. CMV and TB may also co-infect the same child. The aim of this study is to compare the impact on 15-day and 1-year mortality of empirical treatment against TB and CMV plus standard of care (SoC) versus SoC in HIV-infected infants with severe pneumonia.
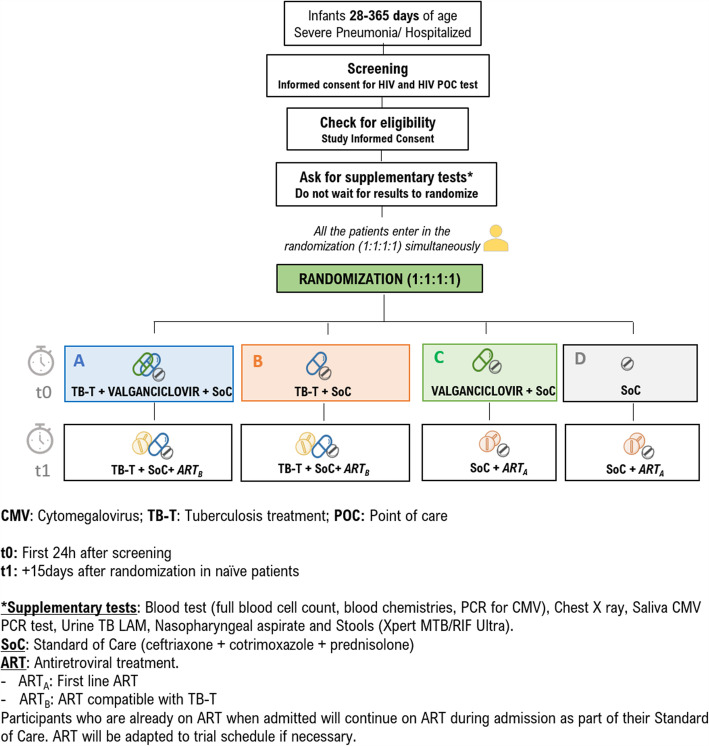
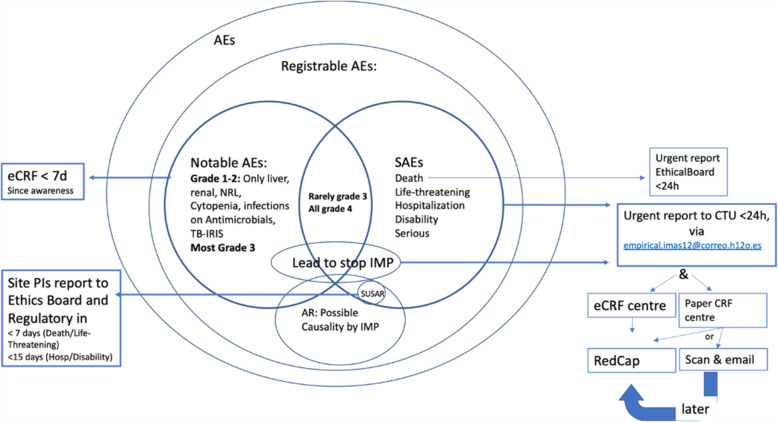
This is a Phase II-III, open-label randomized factorial (2 × 2) clinical trial, conducted in six African countries. The trial has four arms. Infants from 28 to 365 days of age HIV-infected and hospitalized with severe pneumonia will be randomized (1:1:1:1) to (i) SoC, (ii) valganciclovir, (iii) TB-T, and (iv) TB-T plus valganciclovir. The primary endpoint of the study is all-cause mortality, focusing on the short-term (up to 15 days) and long-term (up to 1 year) mortality. Secondary endpoints include repeat hospitalization, duration of oxygen therapy during initial admission, severe and notable adverse events, adverse reactions, CMV and TB prevalence at enrolment, TB incidence, CMV viral load reduction, and evaluation of diagnostic tests such as GeneXpert Ultra on fecal and nasopharyngeal aspirate samples and urine TB-LAM.
Given the challenges in diagnosing CMV and TB in children and results from previous autopsy studies that show high rates of poly-infection in HIV-infected infants with respiratory disease, this study aims to evaluate a new approach including empirical treatment of CMV and TB for this patient population. The potential downsides of empirical treatment of these conditions include toxicity and medication interactions, which will be evaluated with pharmacokinetics sub-studies.
ClinicalTrials.gov , NCT03915366, Universal Trial Number U111-1231-4736, Pan African Clinical Trial Registry PACTR201994797961340.
在非洲,肺炎是导致 HIV 感染儿童死亡的主要原因,在因严重肺炎住院的婴儿中,死亡率高达 35-40%。细菌病原体和卡氏肺孢子虫是导致肺炎相关死亡的已知原因,但巨细胞病毒(CMV)和结核病(TB)等其他重要原因仍未得到充分认识和治疗。CMV 引起的免疫反应可能与发生 TB 和 TB 疾病进展的风险相关,CMV 可能加速 HIV 和 TB 引起的疾病。微创尸检证实,CMV 和 TB 是 HIV 儿童死亡的未被认识到的原因。CMV 和 TB 也可能同时感染同一儿童。本研究的目的是比较针对 TB 和 CMV 的经验性治疗联合标准治疗(SoC)与仅 SoC 对患有严重肺炎的 HIV 感染婴儿的 15 天和 1 年死亡率的影响。
这是一项在六个非洲国家进行的 II-III 期、开放标签、两因素(2×2)临床试验。该试验有四个组。28 至 365 天龄的 HIV 感染并因严重肺炎住院的婴儿将按 1:1:1:1 的比例随机(i)SoC、(ii)缬更昔洛韦、(iii)TB-T 和(iv)TB-T 加缬更昔洛韦。该研究的主要终点是全因死亡率,重点关注短期(最多 15 天)和长期(最多 1 年)死亡率。次要终点包括重复住院、初始入院期间吸氧时间、严重和显著不良事件、不良反应、入组时 CMV 和 TB 的患病率、TB 发病率、CMV 病毒载量降低,以及粪便和鼻咽抽吸物样本和尿液 TB-LAM 的 GeneXpert Ultra 等诊断检测的评估。
鉴于儿童中 CMV 和 TB 的诊断挑战以及先前尸检研究结果显示,患有呼吸道疾病的 HIV 感染婴儿中存在高比例的混合感染,因此本研究旨在评估一种新方法,包括针对该患者人群的 CMV 和 TB 的经验性治疗。经验性治疗这些疾病的潜在缺点包括毒性和药物相互作用,这将通过药代动力学子研究进行评估。
ClinicalTrials.gov,NCT03915366,通用试验编号 U111-1231-4736,泛非临床试验注册 PACTR201994797961340。