School of Medicine, Dentistry and Biomedical Sciences, Queen's University, Belfast, UK.
Belfast Health and Social Care NHS Trust, Belfast, UK.
Eur Respir J. 2022 Dec 15;60(6). doi: 10.1183/13993003.00660-2022. Print 2022 Dec.
The benefits of specialist assessment and management have yet to be evaluated within the biologic era of UK severe asthma treatment, and potential disparities have not been considered.
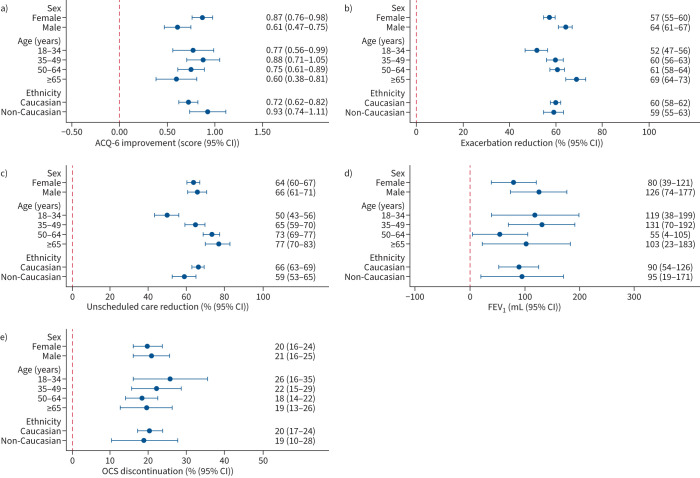
In an uncontrolled before-and-after study, we compared asthma symptoms (Asthma Control Questionnaire-6 (ACQ-6)), exacerbations, unscheduled secondary care use, lung function (forced expiratory volume in 1 s (FEV)) and oral corticosteroid (OCS) dose after 1 year. We compared outcomes by sex, age (18-34, 35-49, 50-64 and ≥65 years), ethnicity (Caucasian non-Caucasian) and hospital site after adjusting for demographics and variation in biologic therapy use.
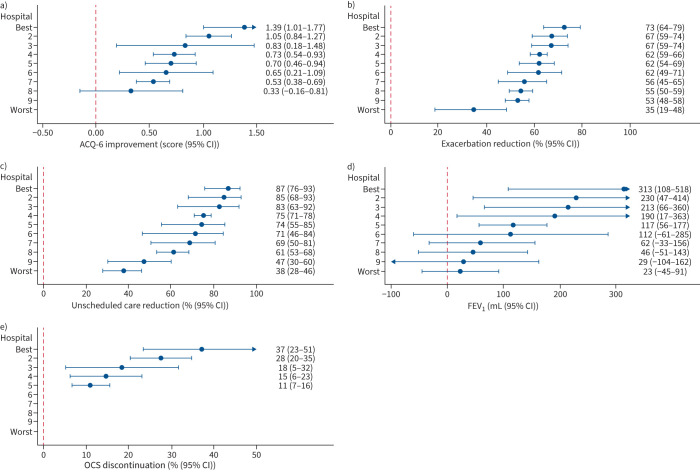
1140 patients were followed-up for 1370 person-years from 12 specialist centres. At annual review, ACQ-6 score was reduced by a median (interquartile range (IQR)) of 0.7 (0.0-1.5), exacerbations by 75% (33-100%) and unscheduled secondary care by 100% (67-100%). FEV increased by a median (IQR) of 20 (-200-340) mL, while OCS dose decreased for 67% of patients. Clinically meaningful improvements occurred across almost all patients, including those not receiving biologic therapy. There was little evidence of differences across demographic groups, although those aged ≥65 years demonstrated larger reductions in exacerbations (69% 52%; p<0.001) and unscheduled care use (77% 50%; p<0.001) compared with patients aged 18-34 years. There were >2-fold differences between the best and worst performing centres across all study outcomes.
Specialist assessment and management is associated with substantially improved patient outcomes, which are broadly consistent across demographic groups and are not restricted to those receiving biologic therapy. Significant variation exists between hospitals, which requires further investigation.
在英国严重哮喘治疗的生物时代,专家评估和管理的益处尚未得到评估,潜在的差异尚未得到考虑。
在一项未经控制的前后对照研究中,我们比较了哮喘症状(哮喘控制问卷-6(ACQ-6))、恶化、非计划性二级护理使用、肺功能(用力呼气量 1 秒(FEV))和口服皮质类固醇(OCS)剂量在 1 年后的变化。我们通过性别、年龄(18-34、35-49、50-64 和≥65 岁)、种族(白种人 非白种人)和医院科室调整人口统计学和生物治疗使用的变化后比较了结果。
从 12 个专科中心随访了 1140 名患者,随访时间为 1370 人年。在年度复查时,ACQ-6 评分中位数(四分位距(IQR))降低了 0.7(0.0-1.5),恶化率降低了 75%(33-100%),非计划性二级护理降低了 100%(67-100%)。FEV 中位数(IQR)增加了 20(-200-340)mL,而 OCS 剂量降低了 67%的患者。几乎所有患者都出现了有临床意义的改善,包括未接受生物治疗的患者。尽管≥65 岁的患者与 18-34 岁的患者相比,恶化(69% 52%;p<0.001)和非计划性护理使用(77% 50%;p<0.001)的降幅更大,但在各人群组之间几乎没有证据表明存在差异。在所有研究结果中,最好和最差表现的中心之间存在 2 倍以上的差异。
专家评估和管理与患者预后的显著改善相关,这些改善在各人群组中基本一致,不限于接受生物治疗的患者。医院之间存在显著差异,需要进一步调查。