Department for Immunology and Inflammation, Centre for Inflammatory Disease, Imperial College London, London, United Kingdom.
Division of Nephrology, University of British Columbia, Vancouver, British Columbia, Canada.
Clin J Am Soc Nephrol. 2022 Jul;17(7):994-1007. doi: 10.2215/CJN.16801221.
C3 glomerulopathy and idiopathic Ig-associated membranoproliferative GN are kidney diseases characterized by abnormal glomerular complement C3 deposition. These conditions are heterogeneous in outcome, but approximately 50% of patients develop kidney failure within 10 years.
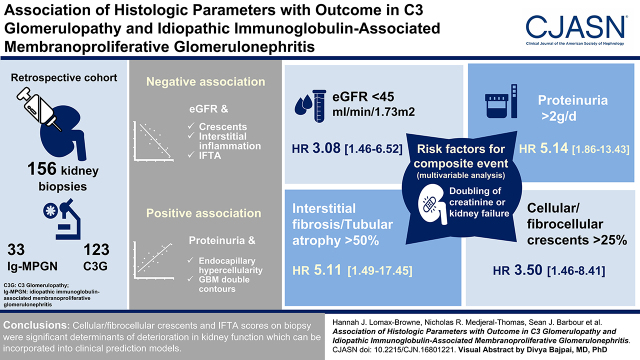
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: To improve identification of patients with poor prognosis, we performed a detailed analysis of percutaneous kidney biopsies in a large cohort of patients. Using a validated histologic scoring system, we analyzed 156 native diagnostic kidney biopsies from a retrospective cohort of 123 patients with C3 glomerulopathy and 33 patients with Ig-associated membranoproliferative GN. We used linear regression, survival analysis, and Cox proportional hazards models to assess the relationship between histologic and clinical parameters with outcome.
Frequent biopsy features were mesangial expansion and hypercellularity, glomerular basement membrane double contours, and endocapillary hypercellularity. Multivariable analysis showed negative associations between eGFR and crescents, interstitial inflammation, and interstitial fibrosis/tubular atrophy. Proteinuria positively associated with endocapillary hypercellularity and glomerular basement membrane double contours. Analysis of second native biopsies did not demonstrate associations between immunosuppression treatment and improvement in histology. Using a composite outcome, risk of progression to kidney failure associated with eGFR and proteinuria at the time of biopsy, cellular/fibrocellular crescents, segmental sclerosis, and interstitial fibrosis/tubular atrophy scores.
Our detailed assessment of kidney biopsy data indicated that cellular/fibrocellular crescents and interstitial fibrosis/tubular atrophy scores were significant determinants of deterioration in kidney function.
C3 肾小球病和特发性 Ig 相关膜增殖性 GN 是肾小球补体 C3 异常沉积的肾脏疾病。这些疾病的预后存在异质性,但约有 50%的患者在 10 年内会发展为肾衰竭。
设计、地点、参与者和测量方法:为了提高对预后不良患者的识别能力,我们对一大组患者的经皮肾活检进行了详细分析。我们使用经过验证的组织学评分系统,分析了来自 C3 肾小球病 123 例患者和 Ig 相关膜增殖性 GN33 例患者的 156 例原发性诊断性肾活检。我们使用线性回归、生存分析和 Cox 比例风险模型来评估组织学和临床参数与预后之间的关系。
活检中常见的特征是系膜扩张和细胞增多、肾小球基底膜双层轮廓和毛细血管内细胞增多。多变量分析显示,eGFR 与新月体、间质炎症和间质纤维化/肾小管萎缩呈负相关。蛋白尿与毛细血管内细胞增多和肾小球基底膜双层轮廓呈正相关。对第二次原发性肾活检的分析并未显示免疫抑制治疗与组织学改善之间存在关联。使用复合结局,与活检时 eGFR 和蛋白尿、细胞/纤维细胞新月体、节段性硬化和间质纤维化/肾小管萎缩评分相关的肾衰竭风险。
我们对肾活检数据的详细评估表明,细胞/纤维细胞新月体和间质纤维化/肾小管萎缩评分是肾功能恶化的重要决定因素。