Centre for Academic Child Health, University of Bristol, Bristol, UK
Centre for Academic Child Health, University of Bristol, Bristol, UK.
BMJ Open. 2022 Jul 1;12(7):e061574. doi: 10.1136/bmjopen-2022-061574.
Conducting randomised controlled trials (RCTs) in primary care is challenging; recruiting patients during time-limited or remote consultations can increase selection bias and physical access to patients' notes is costly and time-consuming. We investigated barriers and facilitators to running a more efficient design.
An RCT aiming to reduce antibiotic prescribing among children presenting with acute cough and a respiratory tract infection (RTI) with a clinician-focused intervention, embedded at the practice level. By using aggregate level, routinely collected data for the coprimary outcomes, we removed the need to recruit individual participants.
Primary care.
Baseline data from general practitioner practices and interviews with individuals from Clinical Research Networks (CRNs) in England who helped recruit practices and Clinical Commission Groups (CCGs) who collected outcome data.
The intervention included: (1) explicit elicitation of parental concerns, (2) a prognostic algorithm to identify children at low risk of hospitalisation and (3) provision of a printout for carers including safety-netting advice.
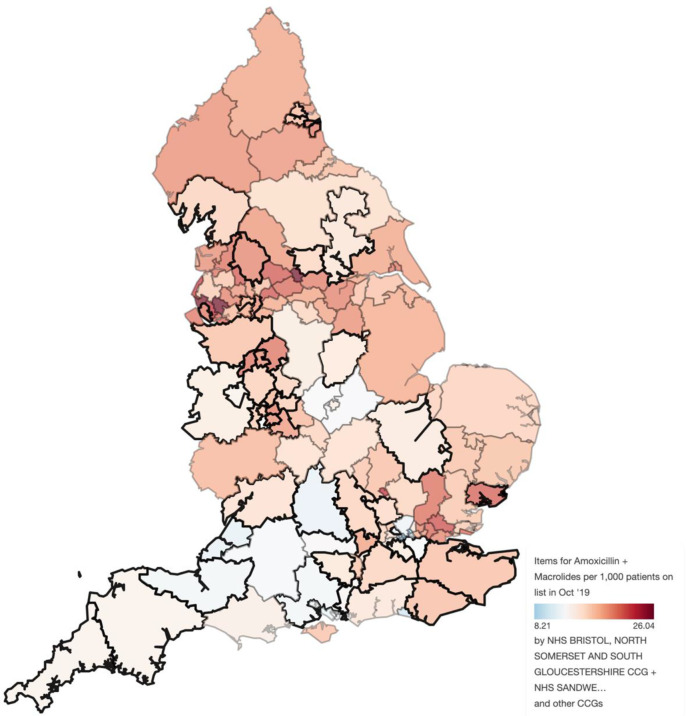
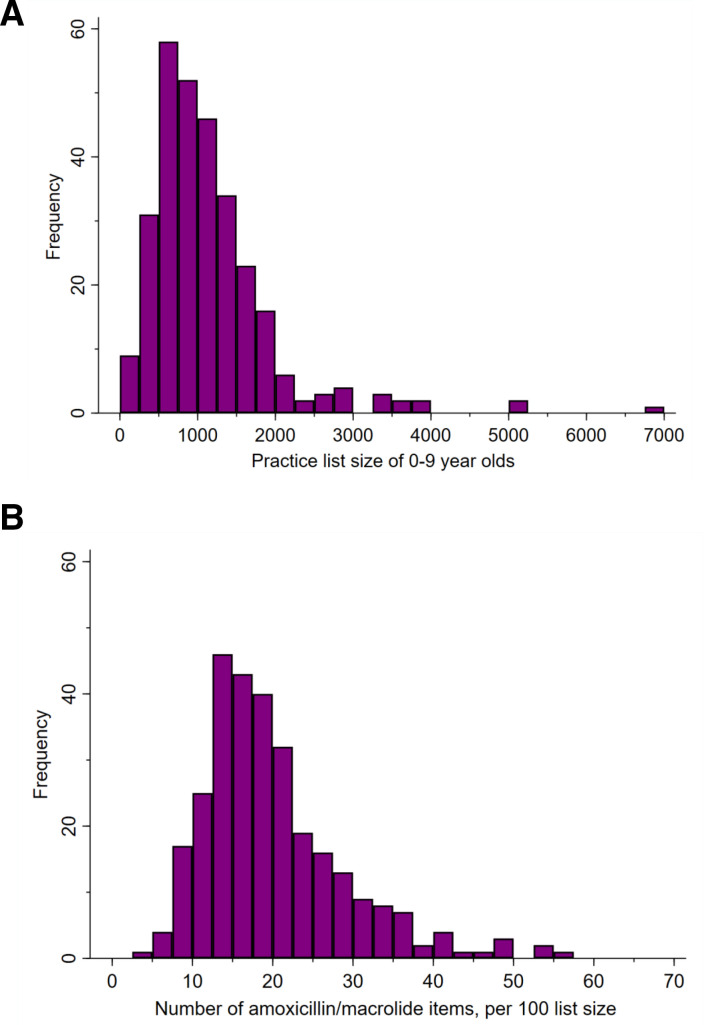
For 0-9 years old-(1) Dispensing data for amoxicillin and macrolide antibiotics and (2) hospital admission rate for RTI.
We recruited 294 of the intended 310 practices (95%) representing 336 496 registered 0-9 years old (5% of all 0-9 years old children). Included practices were slightly larger, had slightly lower baseline prescribing rates and were located in more deprived areas reflecting the national distribution. Engagement with CCGs and their understanding of their role in this research was variable. Engagement with CRNs and installation of the intervention was straight-forward although the impact of updates to practice IT systems and lack of familiarity required extended support in some practices. Data on the coprimary outcomes were almost 100%.
The infrastructure for trials at the practice level using routinely collected data for primary outcomes is viable in England and should be promoted for primary care research where appropriate.
ISRCTN11405239.
在初级保健中进行随机对照试验(RCT)具有挑战性;在限时或远程咨询期间招募患者可能会增加选择偏倚,并且获取患者病历的物理访问既昂贵又耗时。我们研究了提高效率设计的障碍和促进因素。
一项旨在通过以临床医生为重点的干预措施减少因急性咳嗽和呼吸道感染(RTI)就诊的儿童中抗生素处方的 RCT,该研究嵌入在实践层面。通过使用常规收集的汇总水平数据作为主要结局,我们无需招募个体参与者。
初级保健。
来自英格兰临床研究网络(CRN)的个体的基线数据,他们帮助招募实践和收集结局数据的临床委托团体(CCG)。
干预措施包括:(1)明确引出家长的担忧,(2)用于识别低住院风险儿童的预测算法,以及(3)为照顾者提供打印件,包括安全网建议。
对于 0-9 岁儿童-(1) 阿莫西林和大环内酯类抗生素的配药数据,以及 (2) RTI 的住院率。
我们招募了 310 个预定实践中的 294 个(95%),代表了 336496 名登记的 0-9 岁儿童(所有 0-9 岁儿童的 5%)。入选的实践规模稍大,基线处方率稍低,位于更贫困地区,反映了全国的分布情况。与 CCG 的合作及其对其在这项研究中的作用的理解各不相同。与 CRN 的合作和干预措施的实施是直截了当的,尽管由于对实践 IT 系统的更新和缺乏熟悉度的影响,在某些实践中需要扩展支持。主要结局数据几乎达到 100%。
在英格兰,使用常规收集的初级保健研究数据在实践层面进行试验的基础设施是可行的,在适当情况下,应推广用于初级保健研究。
ISRCTN81031274。