Department of Bacteriology and Immunology, University of Helsinki, Helsinki, Finland.
Department of Internal Medicine III, University of Ulm, Ulm, Germany.
Adv Ther. 2022 Sep;39(9):3896-3915. doi: 10.1007/s12325-022-02184-4. Epub 2022 Jul 4.
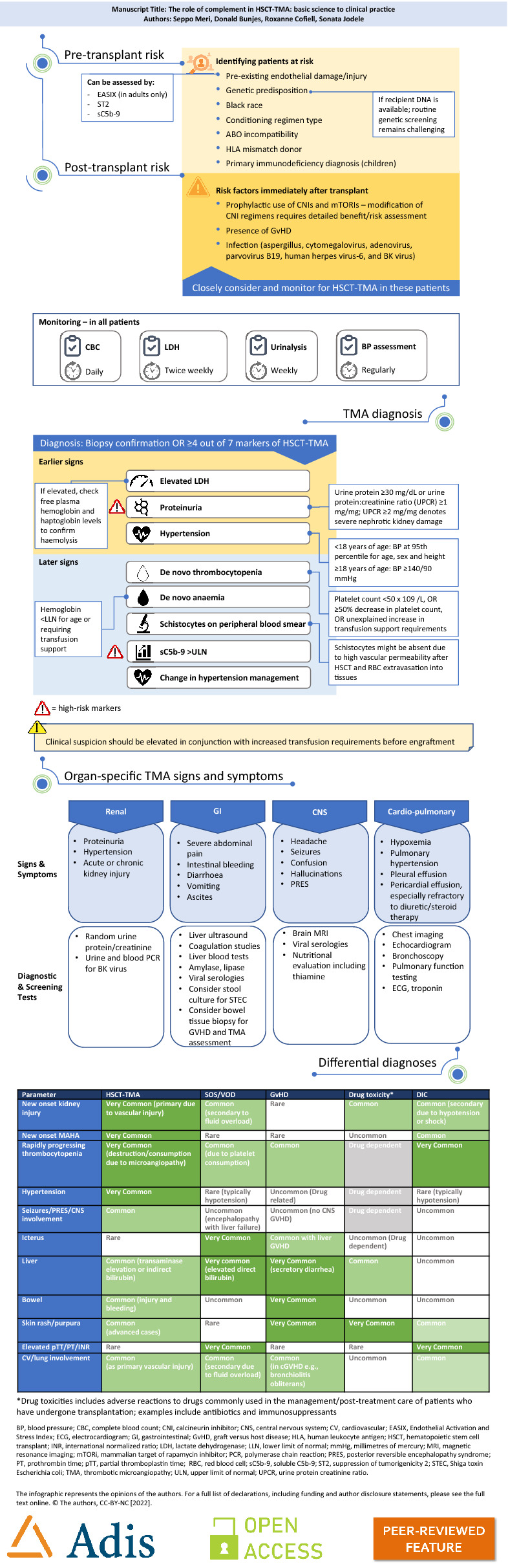
Hematopoietic stem cell transplantation-associated thrombotic microangiopathy (HSCT-TMA) is a common complication occurring post-HSCT and is associated with substantial morbidity and mortality if not promptly identified and treated. Emerging evidence suggests a central role for the complement system in the pathogenesis of HSCT-TMA. The complement system has also been shown to interact with other pathways and processes including coagulation and inflammation, all of which are activated following HSCT. Three endothelial cell-damaging "hits" are required for HSCT-TMA genesis: a genetic predisposition or existing damage, an endothelial cell-damaging conditioning regimen, and additional damaging insults. Numerous risk factors for the development of HSCT-TMA have been identified (including primary diagnosis, graft type, and conditioning regimen) and validated lists of relatively simple diagnostic signs and symptoms exist, many utilizing routine clinical and laboratory assessments. Despite the relative ease with which HSCT-TMA can be screened for, it is often overlooked or masked by other common post-transplant conditions. Recent evidence that patients with HSCT-TMA may also concurrently present with these differential diagnoses only serve to further confound its identification and treatment. HSCT-TMA may be treated, or even prevented, by removing or ameliorating triggering "hits", and recent studies have also shown substantial utility of complement-targeted therapies in this patient population. Further investigation into optimal management and treatment strategies is needed. Greater awareness of TMA post-HSCT is urgently needed to improve patient outcomes; the objective of this article is to clarify current understanding, explain underlying complement biology and provide simple tools to aid the early recognition, management, and monitoring of HSCT-TMA.
造血干细胞移植相关性血栓性微血管病(HSCT-TMA)是一种常见的移植后并发症,如果不能及时发现和治疗,会导致严重的发病率和死亡率。新出现的证据表明,补体系统在 HSCT-TMA 的发病机制中起核心作用。补体系统还与其他途径和过程相互作用,包括凝血和炎症,所有这些在 HSCT 后都会被激活。HSCT-TMA 的发生需要三个内皮细胞损伤的“打击”:遗传易感性或现有损伤、内皮细胞损伤的预处理方案,以及额外的损伤性打击。已经确定了许多与 HSCT-TMA 发展相关的风险因素(包括主要诊断、移植物类型和预处理方案),并且存在相对简单的诊断迹象和症状的验证列表,其中许多利用常规临床和实验室评估。尽管 HSCT-TMA 很容易被筛查出来,但它经常被忽视或被其他常见的移植后疾病所掩盖。最近的证据表明,HSCT-TMA 患者也可能同时存在这些鉴别诊断,这进一步混淆了其识别和治疗。通过去除或改善触发“打击”,HSCT-TMA 可以得到治疗,甚至可以预防,最近的研究还表明,补体靶向治疗在这一患者群体中有很大的应用价值。需要进一步研究最佳管理和治疗策略。迫切需要提高对 HSCT 后 TMA 的认识,以改善患者的预后;本文的目的是澄清目前的认识,解释潜在的补体生物学,并提供简单的工具来帮助早期识别、管理和监测 HSCT-TMA。