Santorsola Mariachiara, Di Lauro Vincenzo, Nasti Guglielmo, Caraglia Michele, Capuozzo Maurizio, Perri Francesco, Cascella Marco, Misso Gabriella, Ottaiano Alessandro
Istituto Nazionale Tumori di Napoli, IRCCS "G. Pascale", Via M. Semmola, 80131 Naples, Italy.
Department of Precision Medicine, University of Campania "L. Vanvitelli", Via L. De Crecchio 7, 80138 Naples, Italy.
Cancers (Basel). 2022 Jul 3;14(13):3262. doi: 10.3390/cancers14133262.
Randomised phase III clinical trials represent a methodological milestone to select effective drugs against metastatic cancers. In this context, and particularly in the efficacy assessment of biologic drugs, the initial metastatic tumour burden is a strong prognostic factor.
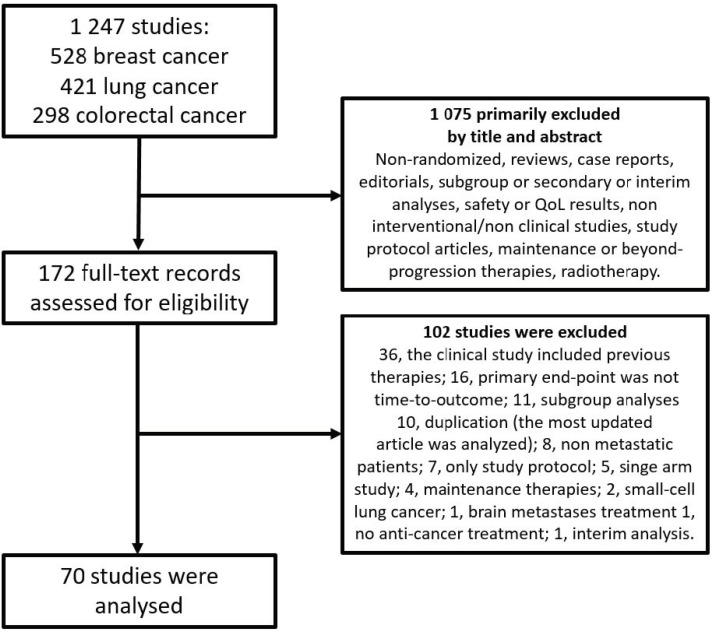
A systematic literature review of randomised, phase III, first-line, clinical trials in metastatic breast, colorectal, and lung cancers, published from 2016 to 2021, was performed. Three groups of variables were collected: identity-, method- (including tumour burden assessment) and outcome-related.
Seventy trials were selected. A large portion of studies (41.4%) focused on the effects of biologic agents (signal inhibitors and immuno-therapies). A definition of low-burden disease based predominantly on the number of involved organs was reported in 28.6% of studies. No explicit reference to oligo-metastatic disease was found either in inclusion/exclusion criteria or in final descriptive data analyses. Disease extent, heterogeneously defined, was a stratification factor for randomisation in only 25.7% of studies. In two studies, a significant imbalance between arms in patients with low-burden disease was revealed.
Attention to initial tumour burden in designing future clinical trials (including the harmonisation of definitions and the reporting of eventual oligo-metastatic disease, complete estimates of tumour volume, and its consideration as a stratification factor) should be increased.
随机III期临床试验是筛选转移性癌症有效药物的方法学里程碑。在此背景下,尤其是在生物药物的疗效评估中,初始转移性肿瘤负荷是一个强有力的预后因素。
对2016年至2021年发表的转移性乳腺癌、结直肠癌和肺癌的随机III期一线临床试验进行系统文献综述。收集了三组变量:身份相关、方法相关(包括肿瘤负荷评估)和结果相关。
共筛选出70项试验。很大一部分研究(41.4%)关注生物制剂(信号抑制剂和免疫疗法)的效果。28.6%的研究报告了主要基于受累器官数量的低负荷疾病定义。在纳入/排除标准或最终描述性数据分析中均未明确提及寡转移疾病。疾病范围定义不统一,仅25.7%的研究将其作为随机分组的分层因素。在两项研究中,发现低负荷疾病患者组间存在显著失衡。
在设计未来的临床试验时,应更多关注初始肿瘤负荷(包括定义的统一、最终寡转移疾病的报告、肿瘤体积的完整估计以及将其作为分层因素)。