Facciorusso Antonio, Mangiavillano Benedetto, Paduano Danilo, Binda Cecilia, Crinò Stefano Francesco, Gkolfakis Paraskevas, Ramai Daryl, Fugazza Alessandro, Tarantino Ilaria, Lisotti Andrea, Fusaroli Pietro, Fabbri Carlo, Anderloni Andrea
Gastroenterology Unit, Department of Surgical and Medical Sciences, University of Foggia, 71122 Foggia, Italy.
Gastroenterology and Digestive Endoscopy Unit, Department of Medicine, The Pancreas Institute, University Hospital of Verona, 37100 Verona, Italy.
Cancers (Basel). 2022 Jul 5;14(13):3291. doi: 10.3390/cancers14133291.
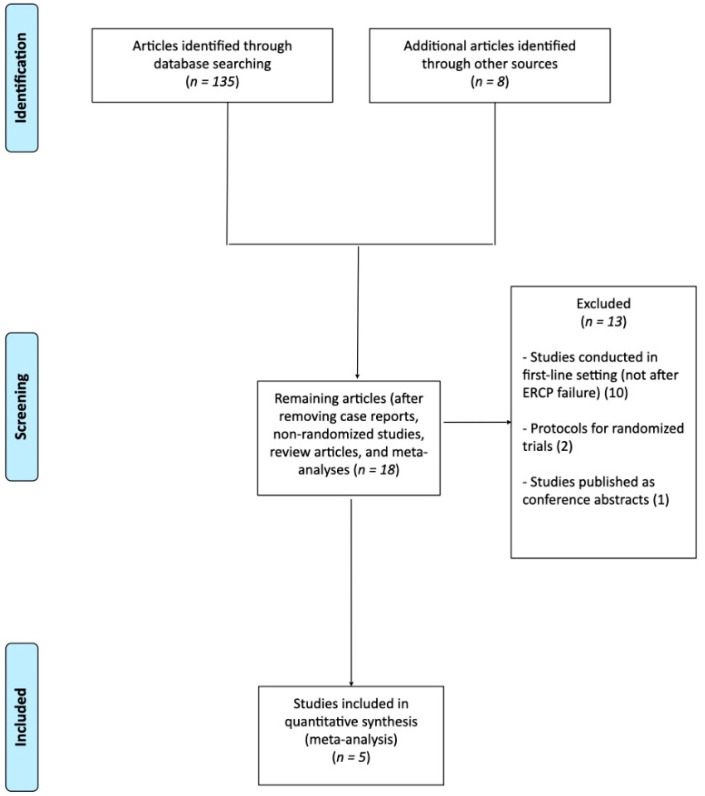
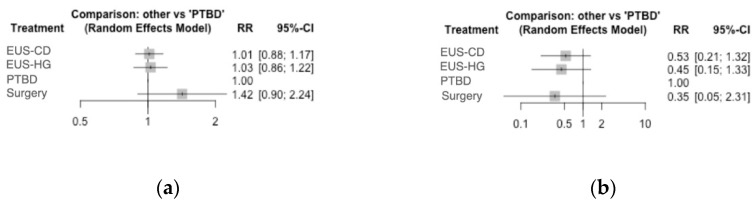
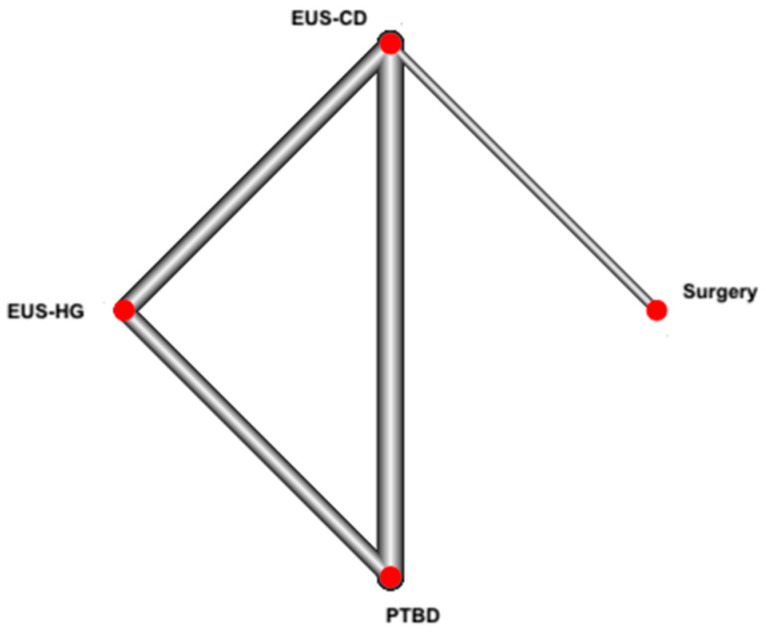
There is scarce evidence on the comparison between different methods for the drainage of distal malignant biliary obstruction (DMBO) after endoscopic retrograde cholangiopancreatography (ERCP) failure. Therefore, we performed a network meta-analysis to compare the outcomes of these techniques. We searched main databases through September 2021 and identified five randomized controlled trials. The primary outcome was clinical success. The secondary outcomes were technical success, overall and serious adverse event rate. Percutaneous trans-hepatic biliary drainage was found to be inferior to other interventions (PTBD: RR 1.01, 0.88-1.17 with EUS-choledochoduodenostomy (EUS-CD); RR 1.03, 0.86-1.22 with EUS-hepaticogastrostomy (EUS-HG); RR 1.42, 0.90-2.24 with surgical hepaticojejunostomy). The comparison between EUS-HG and EUS-CD was not significant (RR 1.01, 0.87-1.17). Surgery was not superior to other interventions (RR 1.40, 0.91-2.13 with EUS-CD and RR 1.38, 0.88-2.16 with EUS-HG). No difference in any of the comparisons concerning adverse event rate was detected, although PTBD showed a slightly poorer performance on ranking analysis (SUCRA score 0.13). In conclusion, all interventions seem to be effective for the drainage of DMBO, although PTBD showed a trend towards higher rates of adverse events.
关于内镜逆行胰胆管造影术(ERCP)失败后远端恶性胆管梗阻(DMBO)不同引流方法之间的比较,几乎没有证据。因此,我们进行了一项网状Meta分析,以比较这些技术的疗效。我们检索了截至2021年9月的主要数据库,确定了五项随机对照试验。主要结局是临床成功。次要结局是技术成功、总体和严重不良事件发生率。发现经皮经肝胆道引流(PTBD)不如其他干预措施(与内镜超声引导下胆总管十二指肠吻合术(EUS-CD)相比,PTBD:RR 1.01,95%置信区间0.88-1.17;与内镜超声引导下肝胃吻合术(EUS-HG)相比,RR 1.03,95%置信区间0.86-1.22;与外科肝空肠吻合术相比,RR 1.42,95%置信区间0.90-2.24)。EUS-HG和EUS-CD之间的比较无显著差异(RR 1.01,95%置信区间0.87-1.17)。外科手术并不优于其他干预措施(与EUS-CD相比,RR 1.40,95%置信区间0.91-2.13;与EUS-HG相比,RR 1.38,95%置信区间0.88-2.16)。尽管PTBD在排序分析中的表现略差(表面累积排序曲线下面积(SUCRA)分数为0.13),但在任何关于不良事件发生率的比较中均未检测到差异。总之,所有干预措施似乎对DMBO引流均有效,尽管PTBD显示出不良事件发生率较高的趋势。