Graduate School of Medicine, Kurume University, Kurume 830-0011, Japan.
Department of Rehabilitation, Japan Community Health Care Organization Saga Central Hospital, Saga 849-8522, Japan.
Nutrients. 2022 Jun 23;14(13):2596. doi: 10.3390/nu14132596.
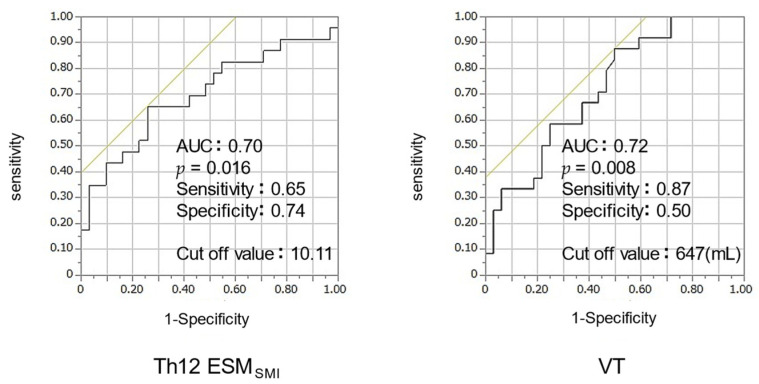
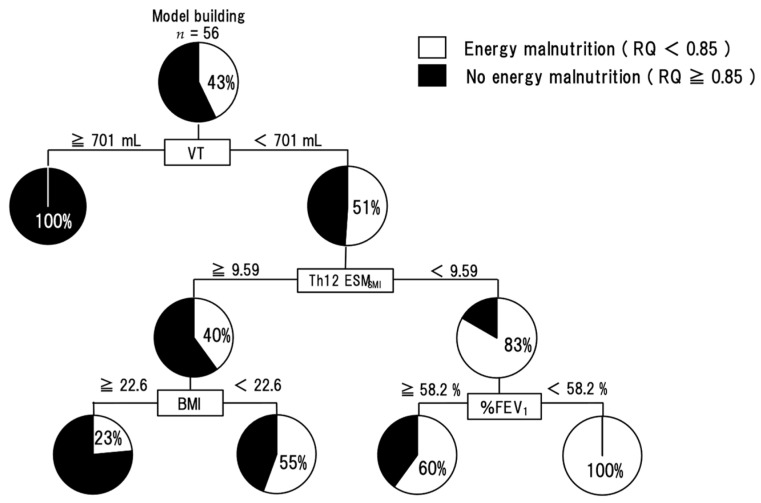
Weight loss is a factor that affects prognosis in patients with chronic obstructive pulmonary disease (COPD) independent of lung function. One of the major factors for weight loss is energy malnutrition. There have been no reports on the factors related to energy malnutrition in COPD patients. This retrospective observational study aimed to investigate these factors. We included 163 male subjects with COPD. Respiratory quotient (RQ), an index of energy malnutrition, was calculated by expiratory gas analysis using an indirect calorimeter. RQ < 0.85 was defined as the energy-malnutrition group and RQ ≥ 0.85 as the no energy-malnutrition group. Factors related to energy malnutrition were examined by multivariate and decision-tree analysis. We finally analyzed data from 56 selected subjects (median age: 74 years, BMI: 22.5 kg/m2). Energy malnutrition was observed in 43%. The independent factors associated with energy malnutrition were tidal volume (VT) (OR 0.99; 95% CI 0.985−0.998; p = 0.015) and Th12 erector spinae muscle cross-sectional area SMI (Th12ESMSMI) (OR 0.71; 95% CI 0.535−0.946; p = 0.019). In decision-tree profiling of energy malnutrition, VT was extracted as the first distinguishable factor, and Th12ESMSMI as the second. In ROC analysis, VT < 647 mL (AUC, 0.72) or Th12ESMSMI < 10.1 (AUC, 0.70) was the cutoff value for energy malnutrition. Energy malnutrition may be an early warning sign of nutritional disorders.
体重减轻是影响慢性阻塞性肺疾病(COPD)患者预后的一个因素,与肺功能无关。体重减轻的主要原因之一是能量营养不良。目前还没有关于 COPD 患者能量营养不良相关因素的报告。这项回顾性观察研究旨在探讨这些因素。我们纳入了 163 名男性 COPD 患者。通过间接热量计使用呼气气体分析计算呼吸商(RQ),这是能量营养不良的一个指标。RQ<0.85 定义为能量营养不良组,RQ≥0.85 定义为无能量营养不良组。通过多变量和决策树分析检查与能量营养不良相关的因素。我们最终分析了 56 名选定患者(中位年龄:74 岁,BMI:22.5kg/m2)的数据。观察到 43%的患者存在能量营养不良。与能量营养不良相关的独立因素是潮气量(VT)(OR 0.99;95%CI 0.985-0.998;p=0.015)和第 12 胸椎竖脊肌横截面积 SMI(Th12ESMSMI)(OR 0.71;95%CI 0.535-0.946;p=0.019)。在能量营养不良的决策树分析中,VT 被提取为第一个可区分的因素,Th12ESMSMI 为第二个。在 ROC 分析中,VT<647mL(AUC,0.72)或 Th12ESMSMI<10.1(AUC,0.70)是能量营养不良的截断值。能量营养不良可能是营养紊乱的早期预警信号。