Ogbue Olisaemeka, Haddad Abdo, Almassi Nima, Lapinski James, Daw Hamed
Department of Medicine, Cleveland Clinic/Fairview Hospital, Cleveland, OH, USA.
Department of Hematology/Oncology, Cleveland Clinic Cancer Center, Cleveland, OH, USA.
Transl Androl Urol. 2022 Jun;11(6):877-901. doi: 10.21037/tau-22-43.
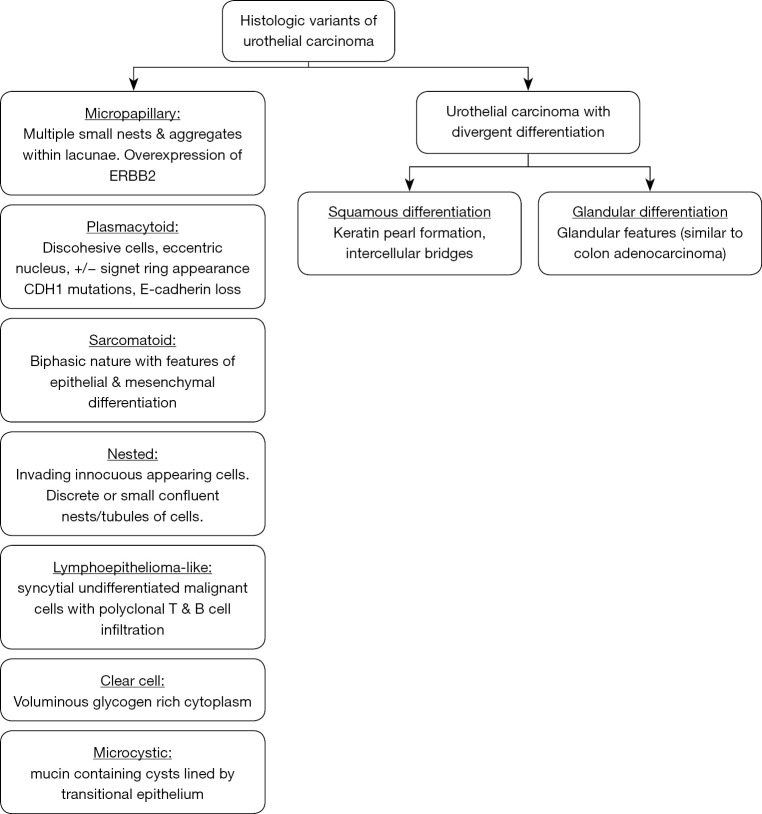
The histologic variants of urothelial carcinoma (UC) are tumors arising from within the urothelium in which some component of the tumor morphology is other than urothelial. They are underdiagnosed, aggressive and have varying pathologic response rates to systemic chemotherapy. There are no consensus guidelines on the use of systemic chemotherapy in variant histology (VH) of UC. We performed a contemporary review on pathologic response rates to neoadjuvant systemic therapy and survival outcomes following radical cystectomy in order to provide a rationale for clinical practice recommendations on the management of UC with VH.
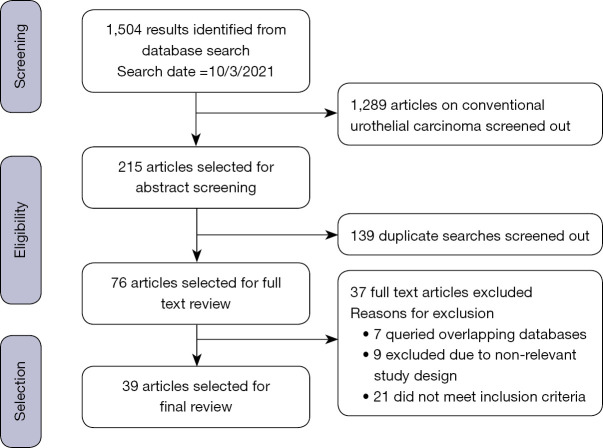
A PubMed literature search was conducted for all English articles from inception reporting either pathological response rates to neoadjuvant treatment or survival outcomes after radical cystectomy in non-metastatic VH of UC.
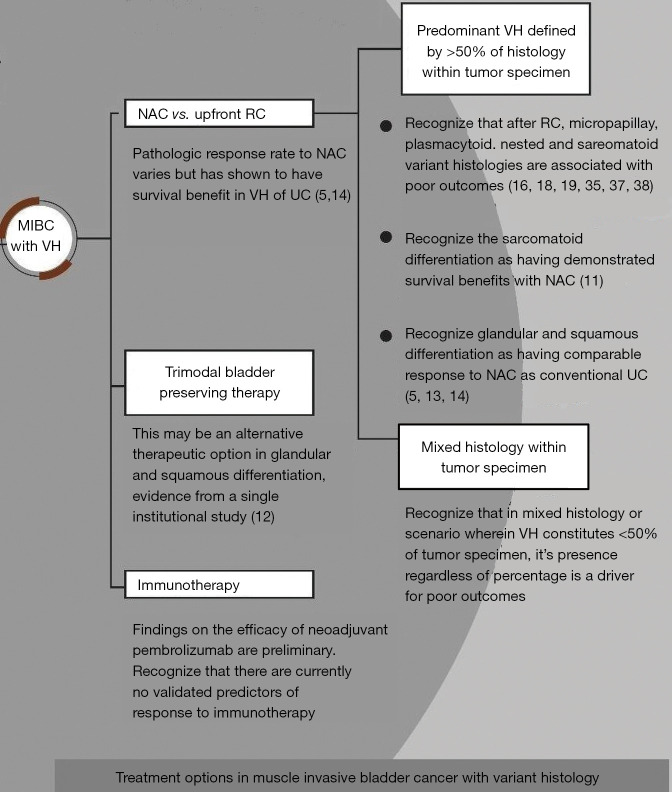
Neoadjuvant chemotherapy (NAC) prior to radical cystectomy was shown to be a beneficial treatment strategy in UC with VH. The micropapillary, plasmacytoid, nested and sarcomatoid histologic variants were associated with worse survival outcomes compared to conventional UC and UC with squamous or glandular differentiation despite initial downstaging with chemotherapy. There is evidence of improved survival in patients with sarcomatoid differentiation receiving NAC compared to RC alone. The major prognostic factors that affect survival outcomes in VH of UC include histologic variant subtype, patient age, presence of lymphovascular invasion, hydronephrosis, nodal metastasis and advanced T stage at diagnosis. Recent studies demonstrate that VH of UC are heterogenous tumors and responsiveness to NAC may be a function of the molecular subtypes present.
Based on these findings, NAC to achieve pathologic downstaging prior to radical cystectomy is recommended for MIBC with VH. Biomarkers identified by molecular profiling with immunohistochemistry will need to be validated as predictors of response to NAC in future trials.
尿路上皮癌(UC)的组织学变异型是起源于尿路上皮的肿瘤,其肿瘤形态的某些成分并非尿路上皮性。它们诊断不足、侵袭性强,对全身化疗的病理反应率各异。对于UC变异型组织学(VH)中全身化疗的应用,尚无共识性指南。我们对新辅助全身治疗的病理反应率以及根治性膀胱切除术后的生存结果进行了当代综述,以便为VH型UC的管理提供临床实践建议的依据。
对PubMed数据库进行文献检索,纳入自数据库建立以来所有报道UC非转移性VH新辅助治疗病理反应率或根治性膀胱切除术后生存结果的英文文章。
根治性膀胱切除术前的新辅助化疗(NAC)被证明是VH型UC的一种有益治疗策略。与传统UC以及伴有鳞状或腺性分化的UC相比,微乳头、浆细胞样、巢状和肉瘤样组织学变异型的生存结果较差,尽管化疗后肿瘤分期有所降低。有证据表明,与单纯根治性膀胱切除术相比,接受NAC的肉瘤样分化患者生存率有所提高。影响UC的VH生存结果的主要预后因素包括组织学变异型亚型、患者年龄、是否存在淋巴管浸润、肾积水、淋巴结转移以及诊断时的T分期。近期研究表明,UC的VH是异质性肿瘤,对NAC的反应性可能是所存在分子亚型的一种功能。
基于这些发现,对于VH型肌层浸润性膀胱癌(MIBC),建议在根治性膀胱切除术前进行NAC以实现病理降期。未来试验中需要验证通过免疫组织化学分子谱分析确定的生物标志物作为NAC反应预测指标的有效性。