Guangdong Lung Cancer Institute, Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China.
School of Medicine, South China University of Technology, Guangzhou, China.
Thorac Cancer. 2022 Sep;13(17):2524-2531. doi: 10.1111/1759-7714.14562. Epub 2022 Jul 12.
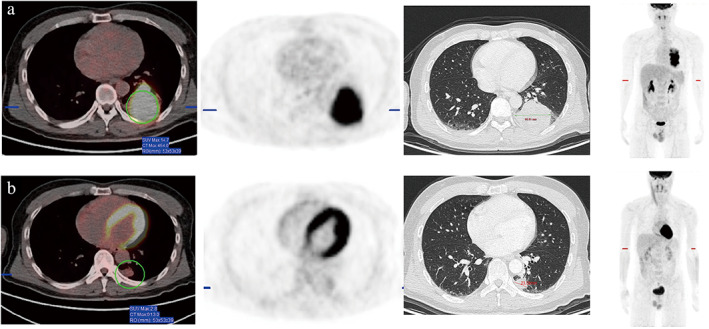
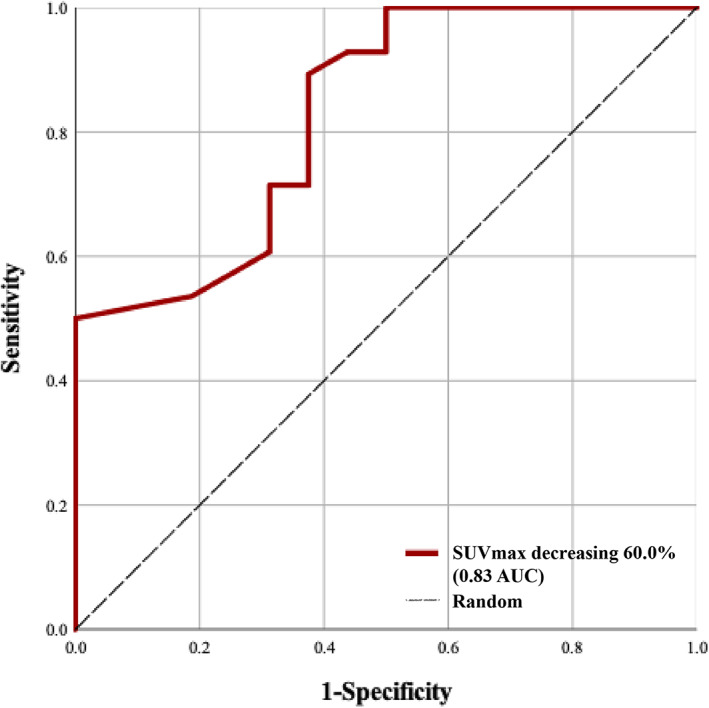
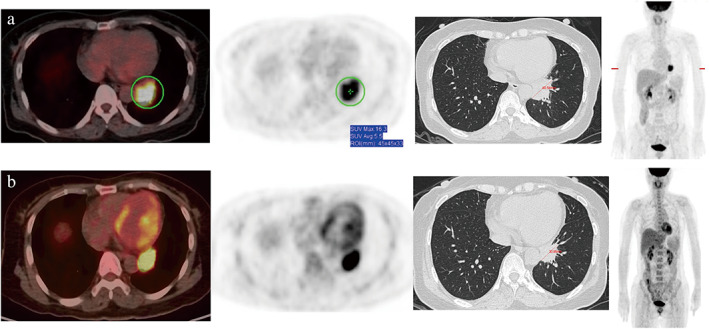
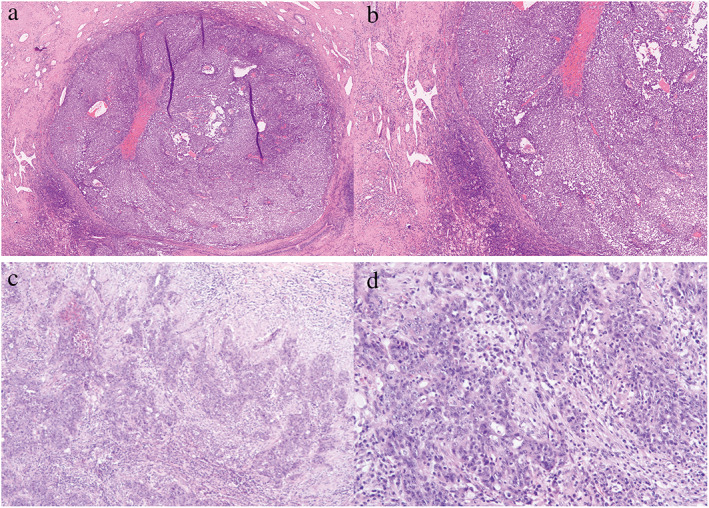
Major pathological response (MPR) is a potential surrogate for overall survival. We determined whether the dynamic changes in F-labeled fluoro-2-deoxyglucose positron emission tomography/computed tomography ( F-FDG PET/CT) were associated with MPR in patients receiving neoadjuvant immunotherapy. Forty-four patients with stage II-III non-small cell lung cancer (NSCLC) who received neoadjuvant immunotherapy and radical surgery were enrolled. Moreover, F-FDG PET/CT scans were performed at baseline and within 1 week before surgery to evaluate the disease. All histological sections were reviewed to assess MPR. The detailed clinical features of the patients were analyzed. The reliability of the clinical variables was assessed in differentiating between MPR and non-MPR using logistic regression. Receiver-operating characteristic (ROC) curve analysis identified the SUVmax changes threshold most associated with MPR. Most of the patients were pathologically diagnosed with squamous cell carcinoma and received anti-PD-1 antibodies plus chemotherapy. The immunotherapy regimens included nivolumab, pembrolizumab, and camrelizumab. MPR was observed in more than half of lesions. Tumors with MPR had a higher decrease in the longest dimension on dynamic PET/CT than those without MPR. Furthermore, the decline in SUVmax was significantly different between MPR and non-MPR diseases, and MPR lesions had a prominent mean reduction in SUVmax. SUVmax reduction was independently associated with MPR in the multivariate regression. On ROC analysis, the threshold of SUVmax decrease in 60% was associated with MPR. Dynamic changes in SUVmax were associated with MPR. The tumors with MPR showed a greater PET/CT response than those without MPR. A SUVmax decrease of more than 60% is more likely to result in an MPR after receiving neoadjuvant immunotherapy.
主要病理反应 (MPR) 是总生存的潜在替代指标。我们确定了接受新辅助免疫治疗的患者中 F-标记的氟代-2-脱氧葡萄糖正电子发射断层扫描/计算机断层扫描 ( F-FDG PET/CT) 的动态变化是否与 MPR 相关。共纳入 44 例接受新辅助免疫治疗和根治性手术的 II-III 期非小细胞肺癌 (NSCLC) 患者。此外,在基线和手术前 1 周内进行 F-FDG PET/CT 扫描以评估疾病。所有组织学切片均进行回顾性评估以评估 MPR。分析患者的详细临床特征。使用逻辑回归评估临床变量在区分 MPR 和非 MPR 方面的可靠性。受试者工作特征 (ROC) 曲线分析确定了与 MPR 最相关的 SUVmax 变化阈值。大多数患者病理诊断为鳞状细胞癌,并接受抗 PD-1 抗体联合化疗。免疫治疗方案包括纳武利尤单抗、帕博利珠单抗和卡瑞利珠单抗。超过一半的病变观察到 MPR。与无 MPR 的肿瘤相比,MPR 肿瘤在动态 PET/CT 上最长径的下降幅度更高。此外,SUVmax 的下降在 MPR 和非 MPR 疾病之间有显著差异,MPR 病变的 SUVmax 均值明显降低。SUVmax 降低在多变量回归中与 MPR 独立相关。在 ROC 分析中,SUVmax 降低 60%的阈值与 MPR 相关。SUVmax 的动态变化与 MPR 相关。MPR 肿瘤比无 MPR 肿瘤具有更大的 PET/CT 反应。接受新辅助免疫治疗后,SUVmax 降低超过 60%更有可能导致 MPR。