Department of Epidemiology and Public Health, Univ Rennes, Rennes University Hospital, F-35000, Rennes, France.
Department of Internal Medicine and Clinical Immunology, Univ Rennes, Rennes University Hospital, F-35000, Rennes, France.
BMC Geriatr. 2022 Jul 13;22(1):576. doi: 10.1186/s12877-022-03192-3.
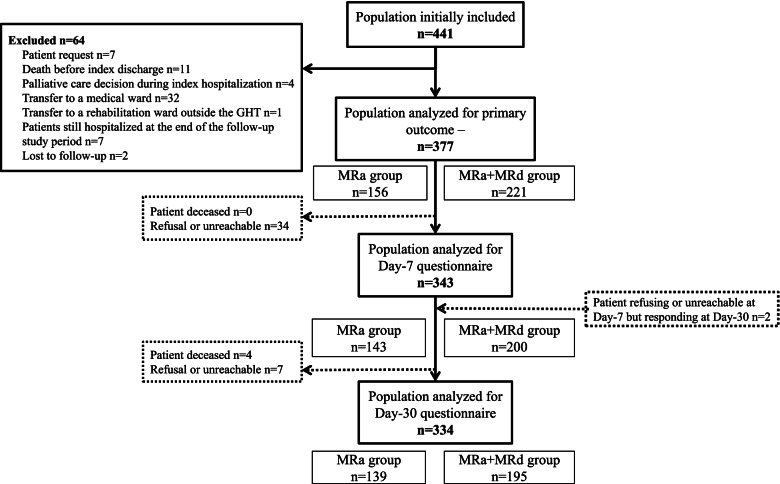
Older patients often experience adverse drug events (ADEs) after discharge that may lead to unplanned readmission. Medication Reconciliation (MR) reduces medication errors that lead to ADEs, but results on healthcare utilization are still controversial. This study aimed to assess the effect of MR at discharge (MRd) provided to patients aged over 65 on their unplanned rehospitalization within 30 days and on both patients' experience of discharge and their knowledge of their medication.
An observational multicenter prospective study was conducted in 5 hospitals in Brittany, France.
Patients who received both MR on admission (MRa) and MRd did not have significantly fewer deaths, unplanned rehospitalizations and/or emergency visits related to ADEs (OR = 1.6 [0.7 to 3.6]) or whatever the cause (p = 0.960) 30 days after discharge than patients receiving MRa alone. However, patients receiving both MRa and MRd were more likely to feel that their discharge from the hospital was well organized (p = 0.003) and reported more frequently that their community pharmacist received information about their hospital stay (p = 0.036).
This study found no effect of MRd on healthcare utilization 30 days after discharge in patients over 65, but the process improved patients' experiences of care continuity. Further studies are needed to better understand this positive impact on their drug care pathway in order to improve patients' ownership of their drugs, which is still insufficient. Improving both the interview step between pharmacist and patient before discharge and the transmission of information from the hospital to primary care professionals is needed to enhance MR effectiveness.
NCT04018781 July 15, 2019.
老年患者出院后常发生药物不良反应(ADE),可能导致非计划性再入院。药物重整(MR)可减少导致 ADE 的用药错误,但对医疗保健利用的影响仍存在争议。本研究旨在评估为 65 岁以上患者在出院时提供的 MR(MRd)对其在 30 天内非计划性再入院的影响,以及对患者出院体验和药物知识的影响。
本研究为在法国布列塔尼的 5 家医院进行的观察性多中心前瞻性研究。
与仅接受入院时 MR(MRa)的患者相比,同时接受 MRa 和 MRd 的患者在出院后 30 天内因 ADE 或任何原因导致的死亡、非计划性再入院和/或急诊就诊(OR=1.6 [0.7 至 3.6])无显著减少(p=0.960)。然而,同时接受 MRa 和 MRd 的患者更有可能认为他们的出院过程组织良好(p=0.003),并且更频繁地报告他们的社区药剂师收到了有关他们住院的信息(p=0.036)。
本研究未发现 65 岁以上患者出院后 30 天内 MRd 对医疗保健利用的影响,但该过程改善了患者对医疗连续性的体验。需要进一步的研究来更好地理解这对他们药物治疗途径的积极影响,以便改善患者对药物的所有权,而这方面仍然不足。需要改进药剂师和患者在出院前的访谈步骤以及从医院向初级保健专业人员传递信息,以提高 MR 的效果。
NCT04018781 2019 年 7 月 15 日。