Dana-Farber Cancer Institute, 450 Brookline Avenue, Boston, MA, 02215, USA.
US Oncology, Texas Oncology, Dallas, TX, USA.
BMC Health Serv Res. 2022 Jul 14;22(1):916. doi: 10.1186/s12913-022-08274-x.
Cabazitaxel significantly improves clinical outcomes compared with a second androgen receptor-targeted agent (ARTA) in patients with metastatic castration-resistant prostate cancer (mCRPC) previously treated with docetaxel and an ARTA (abiraterone or enzalutamide), as demonstrated in the CARD trial (NCT02485691). We aimed to estimate healthcare costs avoided with the use of cabazitaxel as a third-line (3 L) treatment versus a second ARTA from a US payer perspective.
Model inputs were based on the CARD trial, published sources, and estimates of typical clinical care patterns by genitourinary oncologists (n = 3). Assessed time points were 6, 12, 18, and 24 months. Outcomes included progression-free survival (PFS), radiographic PFS (rPFS), and overall survival (OS); hospitalization and intensive care unit (ICU) days; and costs (reported in 2020 US dollar [USD] and converted into Euro) to manage symptomatic skeletal events (SSEs), adverse events (AEs), and end-of-life care.
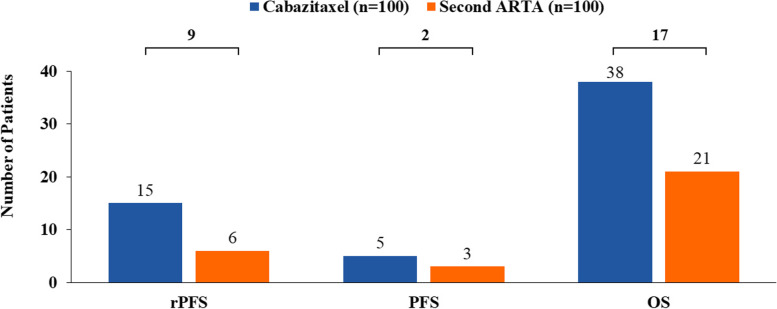
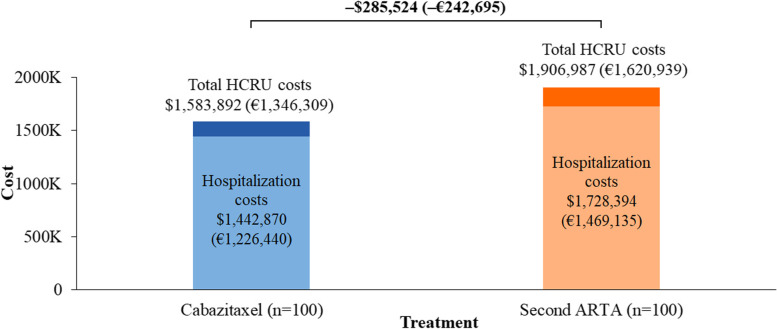
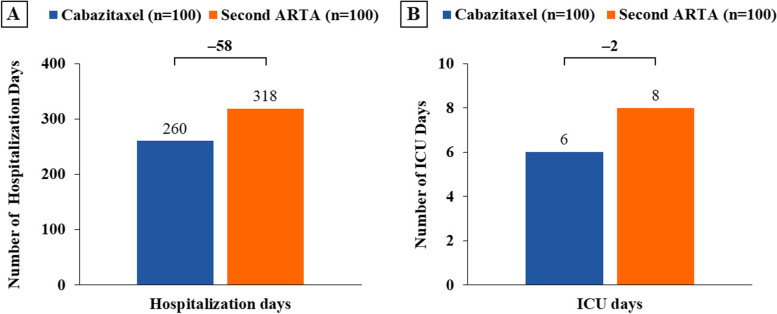
At 18 months, in a cohort of 100 patients, the use of cabazitaxel was estimated to result in 9 more patients achieving rPFS, 2 more patients achieving PFS, and 17 more survivors versus a second ARTA. The costs of SSEs, AEs, and end-of-life care were $498,909 (€424,073), $276,198 (€234,768), and $808,785 (€687,468), respectively, for cabazitaxel and $627,569 (€533,434), $251,124 (€213,455), and $1,028,294 (€874,050), respectively, for a second ARTA. Cabazitaxel was estimated to be associated with a 21% reduction in both SSE management and end-of-life care costs. Hospitalization cost was $1,442,870 (€1,226,440) for cabazitaxel and $1,728,394 (€1,469,135) for a second ARTA, representing an estimated 17% reduction in these costs. Cabazitaxel, as compared with a second ARTA, was associated with 58 fewer hospitalization days and 2 fewer ICU days and was estimated to avoid $323,095 (€274,630, 17%) in total costs, driven by SSEs management and end-of-life care.
The use of cabazitaxel as a 3 L treatment after docetaxel and an ARTA in patients with mCRPC is estimated to result in clinical benefits (longer rPFS, PFS, and OS) and lower healthcare resource utilization (fewer hospitalization and ICU days), compared with a second ARTA.
在先前接受过多西他赛和第二代抗雄激素靶向药物(ARTA)治疗的转移性去势抵抗性前列腺癌(mCRPC)患者中,卡巴他赛与第二代 ARTA(阿比特龙或恩扎鲁胺)相比,显著改善了临床结局,这在 CARD 试验(NCT02485691)中得到了证实。我们旨在从美国支付者的角度评估使用卡巴他赛作为三线(3L)治疗方案相较于第二代 ARTA 可避免的医疗保健成本。
模型输入基于 CARD 试验、已发表的资源以及泌尿科肿瘤学家对典型临床护理模式的估计(n=3)。评估的时间点为 6、12、18 和 24 个月。结果包括无进展生存期(PFS)、放射学无进展生存期(rPFS)和总生存期(OS);住院和重症监护病房(ICU)天数;以及管理症状性骨骼事件(SSEs)、不良事件(AEs)和生命终末期护理的成本(以 2020 年美元(USD)报告并转换为欧元)。
在 18 个月时,在 100 名患者的队列中,与第二代 ARTA 相比,使用卡巴他赛估计可使 9 名患者实现 rPFS、2 名患者实现 PFS 以及 17 名患者存活。SSEs、AEs 和生命终末期护理的成本分别为卡巴他赛的 498,909 美元(424,073 欧元)、276,198 美元(234,768 欧元)和 808,785 美元(687,468 欧元),以及第二代 ARTA 的 627,569 美元(533,434 欧元)、251,124 美元(213,455 欧元)和 1,028,294 美元(874,050 欧元)。卡巴他赛与 SSE 管理和生命终末期护理成本降低 21%相关。卡巴他赛的住院费用为 1,442,870 美元(1,226,440 欧元),第二代 ARTA 的住院费用为 1,728,394 美元(1,469,135 欧元),这些费用预计会降低 17%。与第二代 ARTA 相比,卡巴他赛的住院天数减少了 58 天,重症监护病房天数减少了 2 天,并且由于 SSEs 管理和生命终末期护理,预计可避免 323,095 美元(274,630 欧元,17%)的总成本。
在先前接受过多西他赛和第二代 ARTA 治疗的 mCRPC 患者中,卡巴他赛作为三线治疗方案的应用,与第二代 ARTA 相比,预计可带来临床获益(更长的 rPFS、PFS 和 OS),并降低医疗资源的利用(住院和 ICU 天数更少)。