Center for Innovative Clinical Medicine, Okayama University Hospital, Okayama.
Department of Thoracic Oncology, Aichi Cancer Center, Nagoya, Aichi.
ESMO Open. 2022 Aug;7(4):100527. doi: 10.1016/j.esmoop.2022.100527. Epub 2022 Jul 14.
Mature progression-free survival (PFS) data from the phase III J-ALEX study showed superiority for alectinib versus crizotinib [hazard ratio (HR) 0.37, 95% confidence interval (CI) 0.26-0.52; median PFS 34.1 versus 10.2 months, respectively] in advanced ALK (anaplastic lymphoma kinase)-positive non-small-cell lung cancer (NSCLC). Overall survival (OS) data were immature (HR 0.80, 99.8799% CI 0.35-1.82) at the time of data cut-off (30 June 2018). We report final OS data after ≥5 years of follow-up.
ALK inhibitor naive Japanese patients who were chemotherapy naive or had received one prior chemotherapy regimen were enrolled. Patients were randomized to receive alectinib 300 mg (n = 103) or crizotinib 250 mg (n = 104) twice daily until progressive disease, unacceptable toxicity, death, or withdrawal. The primary endpoint was independent review facility-assessed PFS, with OS (not fully powered) as a secondary endpoint.
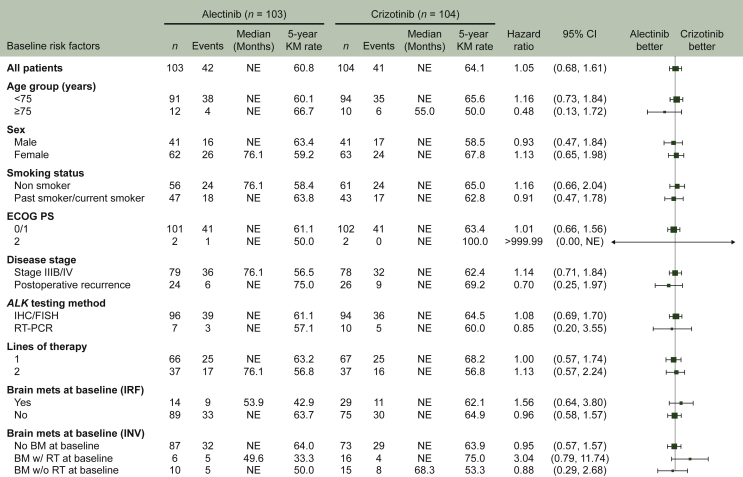
Median duration of OS follow-up was 68.6 months with alectinib and 68.0 months with crizotinib. Treatment with alectinib did not prolong OS relative to crizotinib (HR 1.03, 95.0405% CI 0.67-1.58; P = 0.9105). Five-year OS rates were 60.9% (95% CI 51.4-70.3) with alectinib and 64.1% (95% CI 54.9-73.4) with crizotinib. In total, 91.3% (n = 95/104) of crizotinib-treated patients and 46.6% (n = 48/103) of alectinib-treated patients received at least one subsequent anticancer therapy. After study drug discontinuation, 78.8% of patients in the crizotinib arm switched to alectinib, while 10.7% of patients in the alectinib arm switched to crizotinib as a first subsequent anticancer therapy. Patients randomized to crizotinib tended to switch treatment earlier than those randomized to alectinib.
Final OS analysis from J-ALEX did not show superiority of alectinib to crizotinib; this result was most likely confounded by treatment crossover. Alectinib remains a standard of care for the treatment of patients with advanced ALK-positive NSCLC.
III 期 J-ALEX 研究的成熟无进展生存期(PFS)数据显示,阿来替尼对比克唑替尼具有优越性[风险比(HR)0.37,95%置信区间(CI)0.26-0.52;中位 PFS 分别为 34.1 个月和 10.2 个月],适用于晚期 ALK(间变性淋巴瘤激酶)阳性非小细胞肺癌(NSCLC)患者。在数据截止日期(2018 年 6 月 30 日)时,总生存期(OS)数据尚不成熟(HR 0.80,99.8799%CI 0.35-1.82)。我们报告了≥5 年随访后的最终 OS 数据。
该研究纳入了未经 ALK 抑制剂治疗且化疗初治或仅接受过一次化疗的日本ALK 抑制剂初治患者。患者被随机分配接受阿来替尼 300mg(n=103)或克唑替尼 250mg(n=104),每日两次,直至疾病进展、无法耐受的毒性、死亡或退出。主要终点为独立评估机构评估的 PFS,次要终点为 OS(未完全设盲)。
阿来替尼组和克唑替尼组的中位 OS 随访时间分别为 68.6 个月和 68.0 个月。与克唑替尼相比,阿来替尼并未延长 OS(HR 1.03,95.0405%CI 0.67-1.58;P=0.9105)。阿来替尼组的 5 年 OS 率为 60.9%(95%CI 51.4-70.3),克唑替尼组为 64.1%(95%CI 54.9-73.4)。共有 91.3%(n=95/104)的克唑替尼治疗患者和 46.6%(n=48/103)的阿来替尼治疗患者接受了至少一种后续抗癌治疗。在停止研究药物治疗后,克唑替尼组 78.8%的患者转为接受阿来替尼治疗,而阿来替尼组仅 10.7%的患者转为接受克唑替尼作为首次后续抗癌治疗。随机接受克唑替尼治疗的患者比随机接受阿来替尼治疗的患者更早开始接受治疗转换。
J-ALEX 的最终 OS 分析并未显示阿来替尼优于克唑替尼;这一结果很可能受到治疗交叉的影响。阿来替尼仍然是治疗晚期 ALK 阳性 NSCLC 患者的标准治疗方法。