Tan Jiang-Shan, Liu Ningning, Hu Song, Wu Yan, Gao Xin, Guo Ting-Ting, Yan Xin-Xin, Peng Fu-Hua, Hua Lu
Center for Respiratory and Pulmonary Vascular Diseases, Department of Cardiology, Key Laboratory of Pulmonary Vascular Medicine, National Clinical Research Center of Cardiovascular Diseases, State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Peking University Sixth Hospital/Institute of Mental Health, Beijing, China.
Front Cardiovasc Med. 2022 Jun 30;9:880189. doi: 10.3389/fcvm.2022.880189. eCollection 2022.
To explore the comparative clinical efficacy and safety outcomes of anticoagulation before (pre-) or following (post-) thrombolytic therapy in systemic thrombolytic therapy for pulmonary embolism (PE).
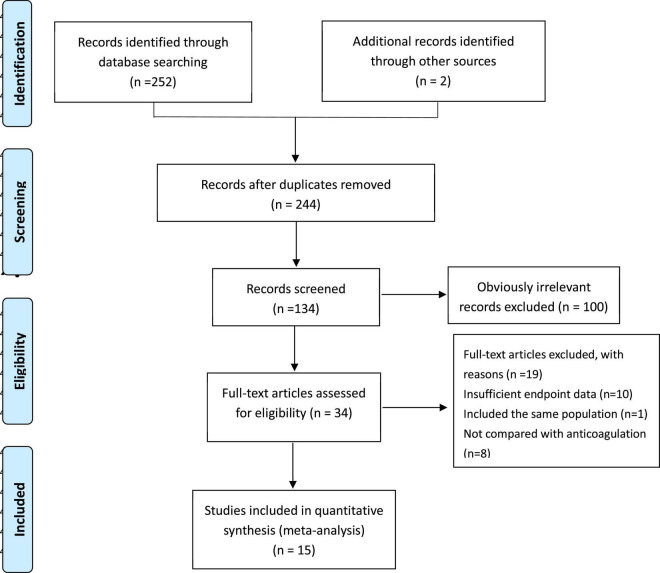
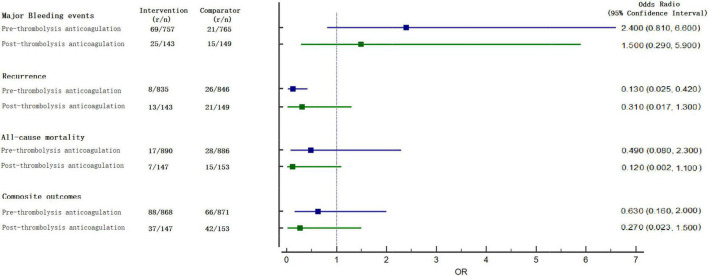
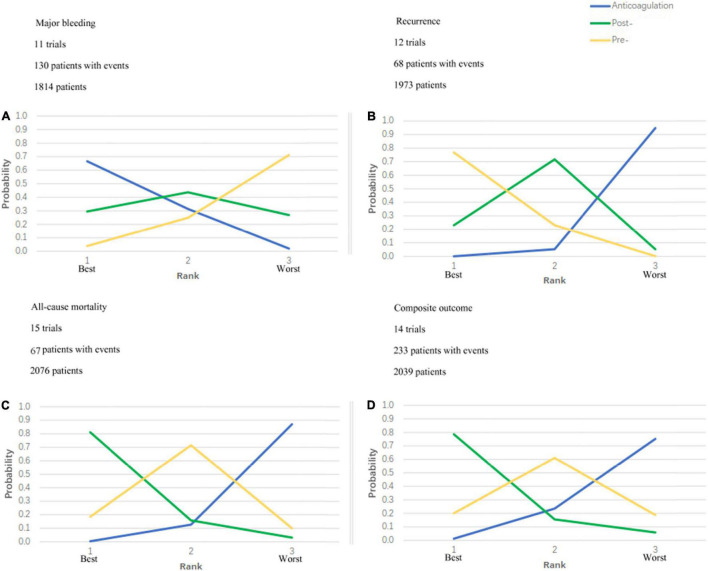
PubMed, the Cochrane Library, EMBASE, EBSCO, Web of Science, and CINAHL databases were searched from inception through 1 May 2021. All randomized clinical trials comparing systemic thrombolytic therapy vs. anticoagulation alone in patients with PE and those that were written in English were eligible. The primary efficacy and safety outcomes were all-cause mortality and major bleeding, respectively. Odds ratios (OR) estimates and associated 95% confidence intervals (CIs) were calculated. A Bayesian network analysis was performed using R studio software, and then the efficacy and safety rankings were derived.
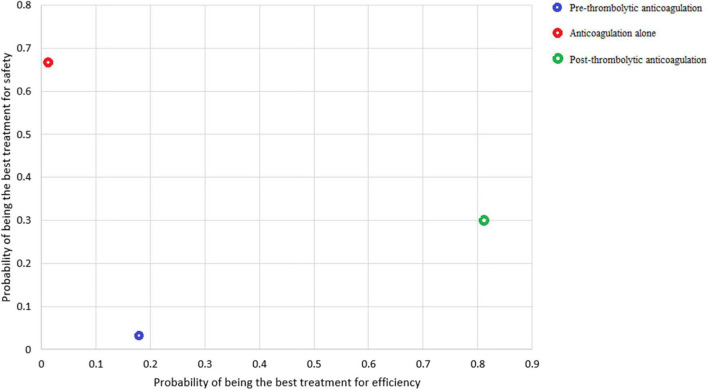
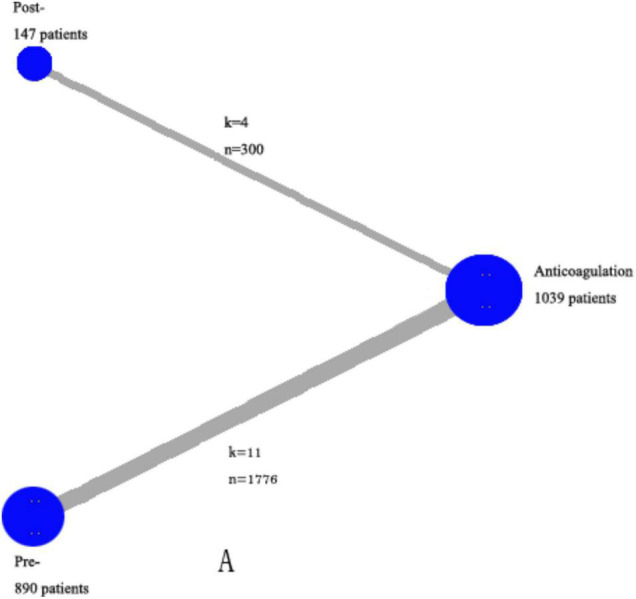
This network meta-analysis enrolled 15 trials randomizing 2,076 patients. According to the plot rankings, the anticoagulant therapy was the best in terms of major bleeding, and the post-thrombolysis anticoagulation was the best in terms of all-cause mortality. Taking major bleeding and all-cause mortality into consideration, the most safe-effective treatment was the post-thrombolysis anticoagulation in patients who needed thrombolytic therapy. The net clinical benefit analysis comparing associated ICH benefits vs. mortality risks of post-thrombolysis anticoagulation demonstrated a net clinical benefit of 1.74%.
The systemic thrombolysis followed by anticoagulation had a better advantage in all-cause mortality and major bleeding than the systemic thrombolysis before anticoagulation. The adjuvant anticoagulation treatment of systemic thrombolytic therapy should be optimized.
探讨在肺栓塞(PE)的全身溶栓治疗中,溶栓治疗前(预)或后(后)进行抗凝治疗的比较临床疗效和安全性结果。
检索了PubMed、Cochrane图书馆、EMBASE、EBSCO、Web of Science和CINAHL数据库,检索时间从数据库建立至2021年5月1日。所有比较PE患者全身溶栓治疗与单独抗凝治疗的随机临床试验以及英文撰写的试验均符合条件。主要疗效和安全性结果分别是全因死亡率和大出血。计算优势比(OR)估计值和相关的95%置信区间(CI)。使用R studio软件进行贝叶斯网络分析,然后得出疗效和安全性排名。
该网络荟萃分析纳入了15项试验,随机分配了2076例患者。根据图表排名,抗凝治疗在大出血方面最佳,溶栓后抗凝在全因死亡率方面最佳。综合考虑大出血和全因死亡率,对于需要溶栓治疗的患者,最安全有效的治疗方法是溶栓后抗凝。比较溶栓后抗凝相关颅内出血益处与死亡风险的净临床效益分析显示净临床效益为1.74%。
溶栓后抗凝在全因死亡率和大出血方面比溶栓前抗凝具有更好的优势。全身溶栓治疗的辅助抗凝治疗应予以优化。