Ge Yunfen, Chen Yue, Hu Zhibin, Mao Hui, Xu Qiong, Wu Qing
Center for Rehabilitation Medicine, Department of Anesthesiology, Zhejiang Provincial People's Hospital (Affiliated People's Hospital, Hangzhou Medical College), Hangzhou, China.
Heart Center, Department of Cardiovascular Surgery, Zhejiang Provincial People's Hospital (Affiliated People's Hospital, Hangzhou Medical College), Hangzhou, China.
Front Surg. 2022 Jun 29;9:934044. doi: 10.3389/fsurg.2022.934044. eCollection 2022.
To evaluate the clinical efficiency of on-table extubation (OTE) versus delayed extubation in patients aged over 60 years that underwent minimally invasive mitral or aortic valve replacement surgery and evaluate the factors associated with successful OTE implementation.
Patients over 60 years with mitral or aortic valve disease who received minimally invasive mitral or aortic valve replacement surgery from October 2020 to October 2021 were selected retrospectively. We divided patients into the on-table extubated (OTE) group ( = 71) and the delayed extubation (DE) group ( = 22). Preoperative, intraoperative, and postoperative clinical variables were compared between the two groups.
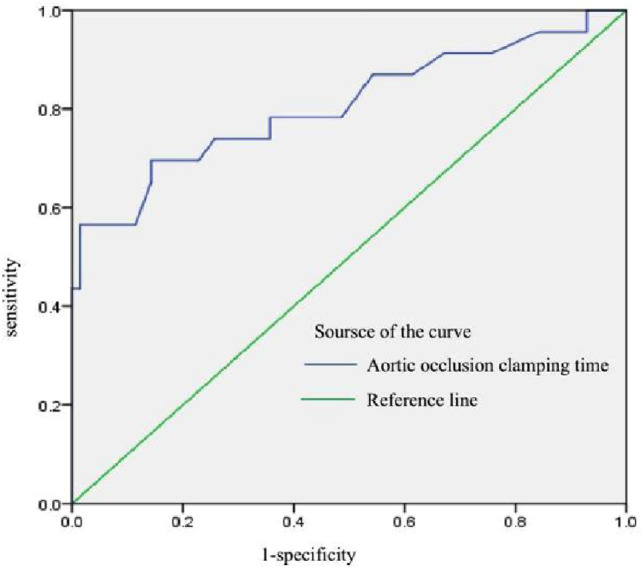
Patients in the DE group underwent longer surgery time, longer aortic occlusion clamping time and longer cardiopulmonary bypass time than those in the OTE group(217.48 ± 27.83 vs 275.91 ± 77.22, = 0.002; 76.49 ± 16.00 vs 126.55 ± 54.85, = 0.001; 112.87 ± 18.91 vs 160.77 ± 52.17, = 0.001). Patients in the OTE group had shorter postoperative mechanical ventilation time (min), shorter ICU time, shorter postoperative hospital length of stay and lower total cost and medication cost ( < 0.05). The AUC for aortic occlusion clamping time was 0.81 ( < 0.01), making it the most significant predictor of on-table extubation success.
On-table extubation following mitral or aortic valve cardiac surgery was associated with a superior clinical outcome and high cost-effectiveness.
评估60岁以上接受微创二尖瓣或主动脉瓣置换手术患者的术中拔管(OTE)与延迟拔管的临床效果,并评估与成功实施OTE相关的因素。
回顾性选取2020年10月至2021年10月期间接受微创二尖瓣或主动脉瓣置换手术的60岁以上二尖瓣或主动脉瓣疾病患者。我们将患者分为术中拔管(OTE)组(n = 71)和延迟拔管(DE)组(n = 22)。比较两组患者术前、术中和术后的临床变量。
DE组患者的手术时间、主动脉阻断钳夹时间和体外循环时间均长于OTE组(217.48 ± 27.83 vs 275.91 ± 77.22,P = 0.002;76.49 ± 16.00 vs 126.55 ± 54.85,P = 0.001;112.87 ± 18.91 vs 160.77 ± 52.17,P = 0.001)。OTE组患者术后机械通气时间更短(分钟)、ICU时间更短、术后住院时间更短且总费用和药物费用更低(P < 0.05)。主动脉阻断钳夹时间的曲线下面积为0.81(P < 0.01),使其成为术中拔管成功的最显著预测因素。
二尖瓣或主动脉瓣心脏手术后的术中拔管与更好的临床结果和高成本效益相关。