Horodyski Laura, Gonzalez Javier, Tabbara Marina M, Gaynor Jeffrey J, Rodriguez-Cabero Maria, Herranz-Amo Felipe, Hernández Carlos, Shah Rushi, Ciancio Gaetano
Department of Urology, University of Miami Miller School of Medicine, Miami, FL, United States.
Servicio de Urologia, Hospital General Universitario Gregorio Marañón, Madrid, Spain.
Front Oncol. 2022 Jun 30;12:877310. doi: 10.3389/fonc.2022.877310. eCollection 2022.
It has been suggested that inferior vena cava (IVC) reconstruction following resection of retroperitoneal tumors with IVC tumor thrombus (TT) is not required when adequate collateral circulation is present. There are no reports evaluating mid-term effects on renal function in these patients. The purpose of this study was to assess renal function after resection of right renal cell carcinoma (RCC) with obstructing IVC TT and the possible risks that may arise after left renal vein division.
A bi-institutional retrospective review was performed over a 15-year period, assessing patients with right RCC and obstructing level II-IV TT. All patients underwent extensive evaluation and cardiology clearance, and informed consent was obtained for right radical nephrectomy and thrombectomy with or without IVC reconstruction with possible cardiopulmonary bypass (CPB). Patient demographics, tumor characteristics, intraoperative factors, complications, length of stay, and patient survival were evaluated. Preoperative creatinine was recorded, as was creatinine on the day of discharge and at 6 and 12 months postoperatively.
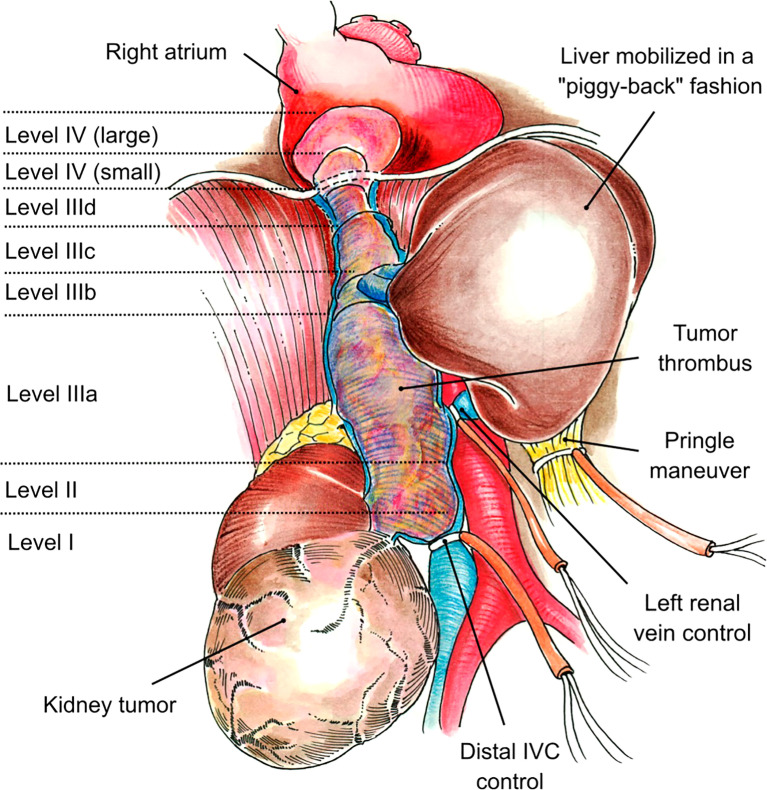
Twenty-two patients were included in the study. Median age at surgery was 62.5 (range: 45-79) years, and 19 (86%) of the patients were men. One patient (5%) had a level II thrombus, 14 patients (64%) had a level III thrombus (IIIa, n = 3; IIIb, n = 6; IIIc, n = 3; IIId, n = 2), and seven patients (32%) had a level IV thrombus. Intraoperatively, median estimated blood loss was 1.35 (range: 0.2-25) L. The median length of hospital stay was 11 (range: 5-50) days. Median preoperative creatinine was 1.20 (range: 0.40-2.70) mg/dl, and postoperatively, median creatinine was 1.3 (range: 0.86-2.20) mg/dl. Median creatinine levels at 6 months and 12 months postoperatively were 1.10 (range: 0.5-1.8) mg/dl and 1.40 (range: 0.6-2.0) mg/dl, respectively. Four patients died (range: 0.1-1.3 years), and median postoperative follow-up among the 18 ongoing survivors (at last follow-up) was 1.5 (range: 0.5-7.0) years.
Resection of right RCC with an obstructing level II-IV TT without reconstruction of the IVC appears to not have a significant adverse effect on mid-term renal function after division of the left renal vein.
有人提出,当存在足够的侧支循环时,切除伴有下腔静脉(IVC)肿瘤血栓(TT)的腹膜后肿瘤后无需进行IVC重建。目前尚无评估这些患者中期肾功能影响的报告。本研究的目的是评估切除伴有阻塞性IVC TT的右肾细胞癌(RCC)后的肾功能,以及左肾静脉离断后可能出现的风险。
进行了一项为期15年的双机构回顾性研究,评估患有右RCC和阻塞性II-IV级TT的患者。所有患者均接受了全面评估和心脏科检查,并获得了关于右根治性肾切除术和血栓切除术(伴或不伴可能需要体外循环(CPB)的IVC重建)的知情同意书。评估了患者的人口统计学特征、肿瘤特征、术中因素、并发症、住院时间和患者生存率。记录了术前肌酐水平,以及出院当天、术后6个月和12个月的肌酐水平。
本研究纳入了22例患者。手术时的中位年龄为62.5岁(范围:45-79岁),其中19例(86%)为男性。1例患者(5%)有II级血栓,14例患者(64%)有III级血栓(IIIa,n = 3;IIIb,n = 6;IIIc,n = 3;IIId,n = 2),7例患者(32%)有IV级血栓。术中,估计中位失血量为1.35 L(范围:0.2-25 L)。中位住院时间为11天(范围:5-50天)。术前中位肌酐为1.20 mg/dl(范围:0.40-2.70 mg/dl),术后中位肌酐为1.3 mg/dl(范围:0.86-2.20 mg/dl)。术后6个月和12个月的中位肌酐水平分别为1.10 mg/dl(范围:0.5-1.8 mg/dl)和1.40 mg/dl(范围:0.6-2.0 mg/dl)。4例患者死亡(范围:0.1-1.3年),18例存活患者(最后一次随访时)的术后中位随访时间为1.5年(范围:0.5-7.0年)。
切除伴有阻塞性II-IV级TT的右RCC且不进行IVC重建,在离断左肾静脉后似乎对中期肾功能没有显著不良影响。