Division of Surgery, Department of Clinical Science, Intervention and Technology, Karolinska Institutet, Karolinska University Hospital, Stockholm, Sweden.
Department of Biomedical and Clinical Sciences, Division of Surgery, Linköping University, Linköping, Sweden.
BJS Open. 2022 Jul 7;6(4). doi: 10.1093/bjsopen/zrac097.
Post-hepatectomy liver failure (PHLF) is one of the most serious postoperative complications after hepatectomy. The aim of this study was to assess the impact of the International Study Group of Liver Surgery (ISGLS) definition of PHLF on morbidity and short- and long-term survival after major hepatectomy.
This was a retrospective review of all patients who underwent major hepatectomy (three or more liver segments) for various liver tumours between 2010 and 2018 at two Swedish tertiary centres for hepatopancreatobiliary surgery. Descriptive statistics, regression models, and survival analyses were used.
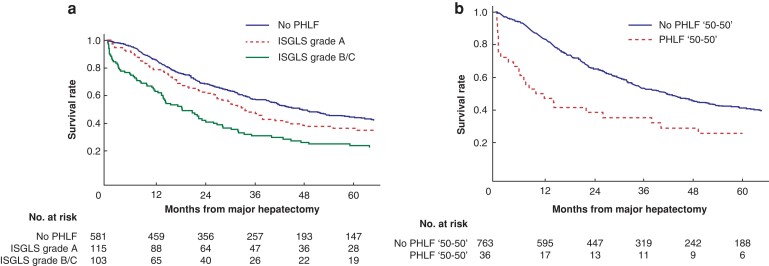
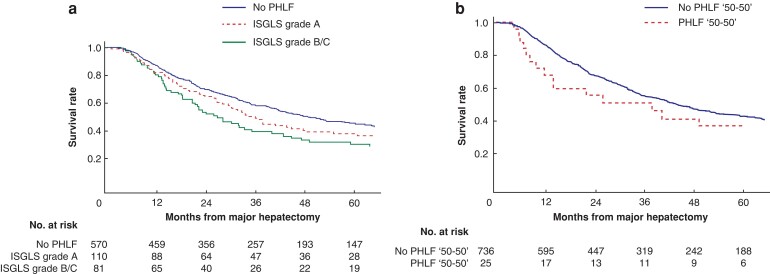
A total of 799 patients underwent major hepatectomy, of which 218 patients (27 per cent) developed ISGLS-defined PHLF, including 115 patients (14 per cent) with ISGLS grade A, 76 patients (10 per cent) with grade B, and 27 patients (3 per cent) with grade C. The presence of cirrhosis, perihilar cholangiocarcinoma, and gallbladder cancer, right-sided hemihepatectomy and trisectionectomy all significantly increased the risk of clinically relevant PHLF (grades B and C). Clinically relevant PHLF increased the risk of 90-day mortality and was associated with impaired long-term survival. ISGLS grade A had more major postoperative complications compared with no PHLF but failed to be an independent predictor of both 90-day mortality and long-term survival. The impact of PHLF grade B/C on long-term survival was no longer present in patients surviving the first 90 days after surgery.
The presently used ISGLS definition for PHLF should be reconsidered regarding mortality as only PHLF grade B/C was associated with a negative impact on short-term survival; however, even ISGLS grade A had clinical implications.
肝切除术后肝功能衰竭(PHLF)是肝切除术后最严重的术后并发症之一。本研究旨在评估国际肝脏外科研究组(ISGLS)对 PHLF 的定义对各种肝脏肿瘤行大范围肝切除术(3 个或以上肝段)后的发病率以及短期和长期生存率的影响。
这是对 2010 年至 2018 年在瑞典两个肝胆胰外科治疗中心接受大范围肝切除术(3 个或以上肝段)的各种肝脏肿瘤患者的回顾性研究。采用描述性统计、回归模型和生存分析。
共 799 例患者行大范围肝切除术,其中 218 例(27%)发生 ISGLS 定义的 PHLF,包括 115 例(14%)ISGLS 分级 A、76 例(10%)ISGLS 分级 B 和 27 例(3%)ISGLS 分级 C。肝硬化、肝门部胆管癌、胆囊癌、右半肝切除术和三叶切除术均显著增加发生临床相关 PHLF(分级 B 和 C)的风险。临床相关 PHLF 增加 90 天死亡率的风险,并与长期生存受损相关。与无 PHLF 相比,ISGLS 分级 A 术后主要并发症更多,但不能独立预测 90 天死亡率和长期生存。在手术后 90 天存活的患者中,PHLF 分级 B/C 对长期生存的影响不再存在。
目前使用的 ISGLS 定义的 PHLF 应重新考虑死亡率,因为只有 PHLF 分级 B/C 与短期生存的负面影响相关;然而,即使是 ISGLS 分级 A 也有临床意义。