Division of Hepato-Biliary-Pancreatic Surgery, Shizuoka Cancer Centre, Shizuoka, Japan.
BJS Open. 2021 Jan 8;5(1). doi: 10.1093/bjsopen/zraa049.
Hepatectomy with extrahepatic bile duct resection is associated with a high risk of posthepatectomy liver failure (PHLF). However, the utility of the remnant liver volume (RLV) in cholangiocarcinoma has not been studied intensively.
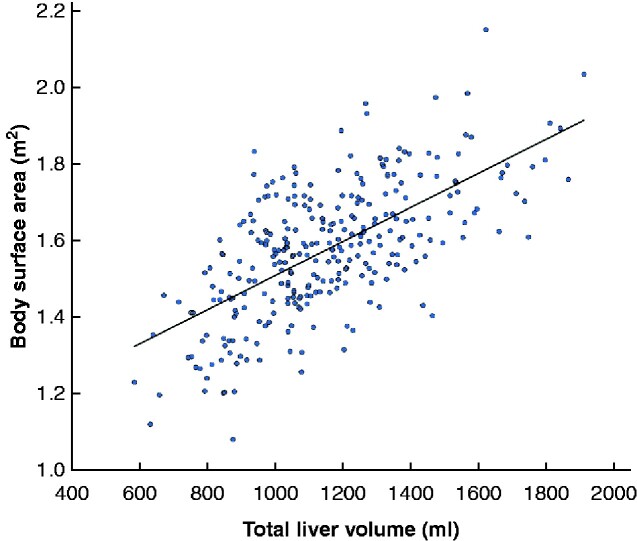
Patients who underwent major hepatectomy with extrahepatic bile duct resection between 2002 and 2018 were reviewed. The RLV was divided by body surface area (BSA) to normalize individual physical differences. Risk factors for clinically relevant PHLF were evaluated with special reference to the RLV/BSA.
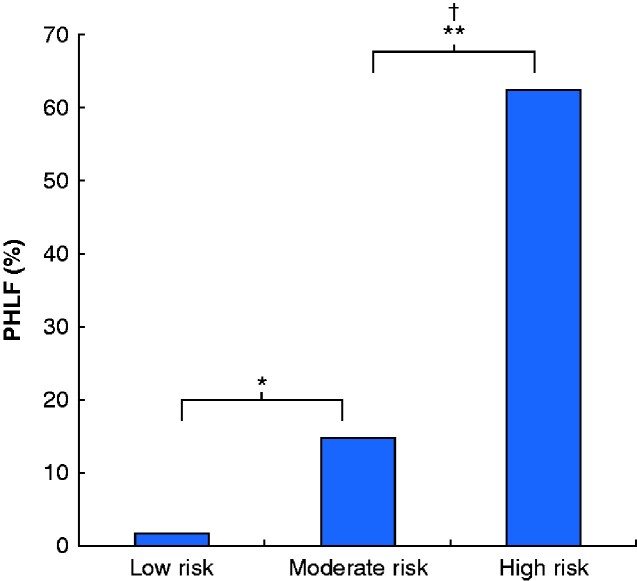
A total of 289 patients were included. The optimal cut-off value for RLV/BSA was determined to be 300 ml/m2. Thirty-two patients (11.1 per cent) developed PHLF. PHLF was more frequent in patients with an RLV/BSA below 300 ml/m2 than in those with a value of 300 ml/m2 or greater: 19 of 87 (22 per cent) versus 13 of 202 (6.4 per cent) (P < 0.001). In multivariable analysis, RLV/BSA below 300 ml/m2 (P = 0.013), future liver remnant plasma clearance rate of indocyanine green less than 0.075 (P = 0.031), and serum albumin level below 3.5 g/dl (P = 0.015) were identified as independent risk factors for PHLF. Based on these risk factors, patients were classified into three subgroups with low (no factors), moderate (1-2 factors), and high (3 factors) risk of PHLF, with PHLF rates of 1.8, 14.8 and 63 per cent respectively (P < 0.001).
An RLV/BSA of 300 ml/m2 is a simple predictor of PHLF in patients undergoing hepatectomy with extrahepatic bile duct resection.
肝切除术联合肝外胆管切除术与术后肝功能衰竭(posthepatectomy liver failure,PHLF)的发生风险较高相关。然而,肝体积残余率(residual liver volume,RLV)在胆管癌中的应用尚未得到深入研究。
回顾了 2002 年至 2018 年间行大范围肝切除术联合肝外胆管切除术的患者。通过体表面积(body surface area,BSA)对 RLV 进行校正,以标准化个体的身体差异。特别参考 RLV/BSA,评估与临床相关的 PHLF 的风险因素。
共纳入 289 例患者。确定 RLV/BSA 的最佳截断值为 300 ml/m2。32 例(11.1%)发生 PHLF。RLV/BSA 低于 300 ml/m2 的患者发生 PHLF 的频率高于 RLV/BSA 等于或大于 300 ml/m2 的患者:87 例中有 19 例(22%)比 202 例中有 13 例(6.4%)(P<0.001)。多变量分析显示,RLV/BSA 低于 300 ml/m2(P=0.013)、吲哚菁绿未来肝脏残留血浆清除率低于 0.075(P=0.031)和血清白蛋白水平低于 3.5 g/dl(P=0.015)是 PHLF 的独立危险因素。根据这些危险因素,患者被分为低危(无因素)、中危(1-2 个因素)和高危(3 个因素)三个亚组,PHLF 发生率分别为 1.8%、14.8%和 63%(P<0.001)。
RLV/BSA 为 300 ml/m2 是预测行肝切除术联合肝外胆管切除术患者 PHLF 的一个简单指标。