Department of Surgery, McMaster University, Hamilton, Ontario, Canada.
Department of Anesthesia, University of Ottawa, Ottawa, Ontario, Canada.
JAMA Netw Open. 2022 Jul 1;5(7):e2222721. doi: 10.1001/jamanetworkopen.2022.22721.
The recent development of targeted therapy and immunotherapy has made neoadjuvant therapy an attractive option for patients with hepatocellular carcinoma (HCC). However, surgeons are concerned that adverse effects of neoadjuvant therapy with these agents could lead to delayed or even cancelled surgeries.
To summarize the current evidence regarding toxicity profiles for tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs) among patients with HCC.
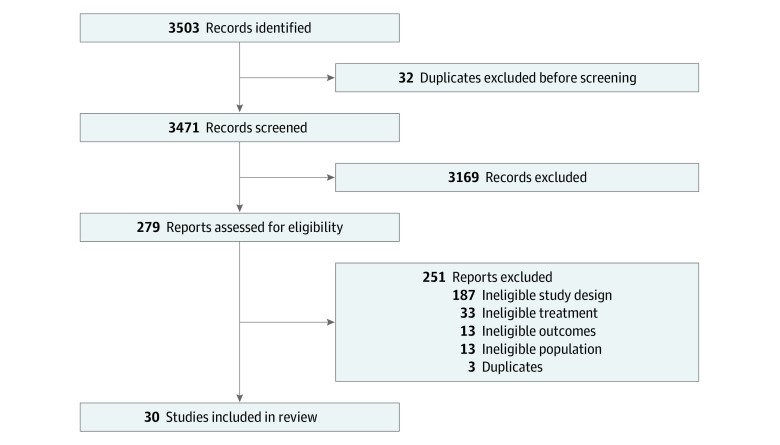
Medline, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) were searched from January 1990 and December 2021.
Single-group, placebo-controlled, and dual-agent clinical trials comparing TKIs and ICIs in patients with HCC were eligible for inclusion.
Following the Preferred Reporting Items in Systematic Reviews and Meta-analysis guideline, 2 reviewers independently extracted data. A random-effects model was used.
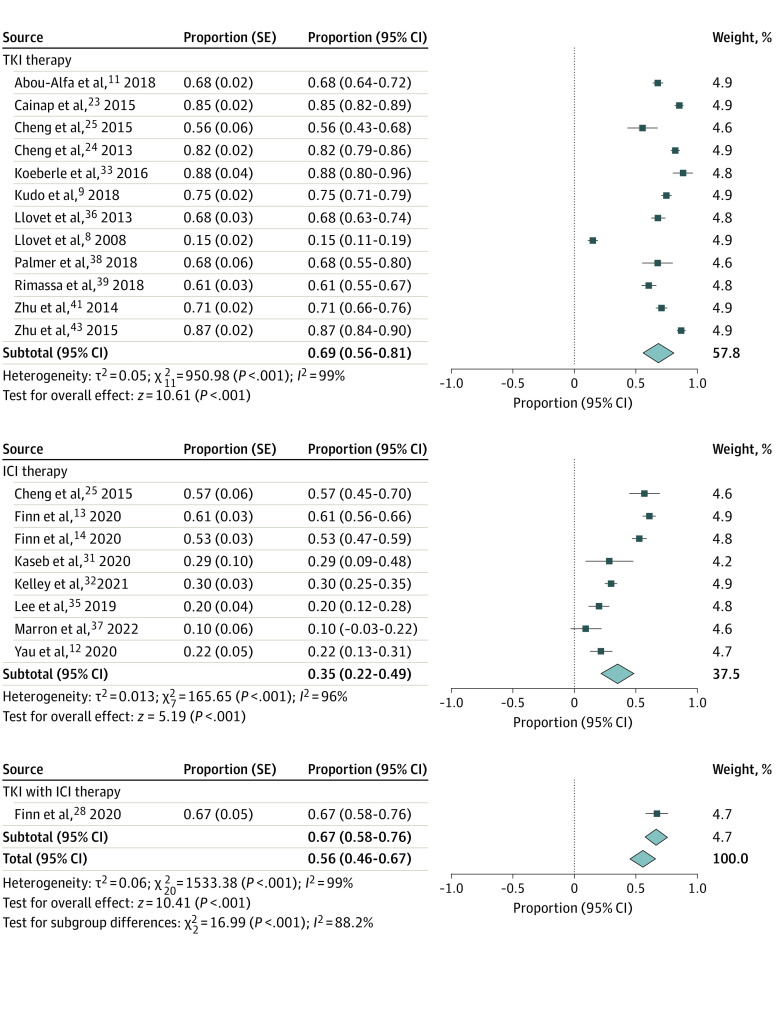
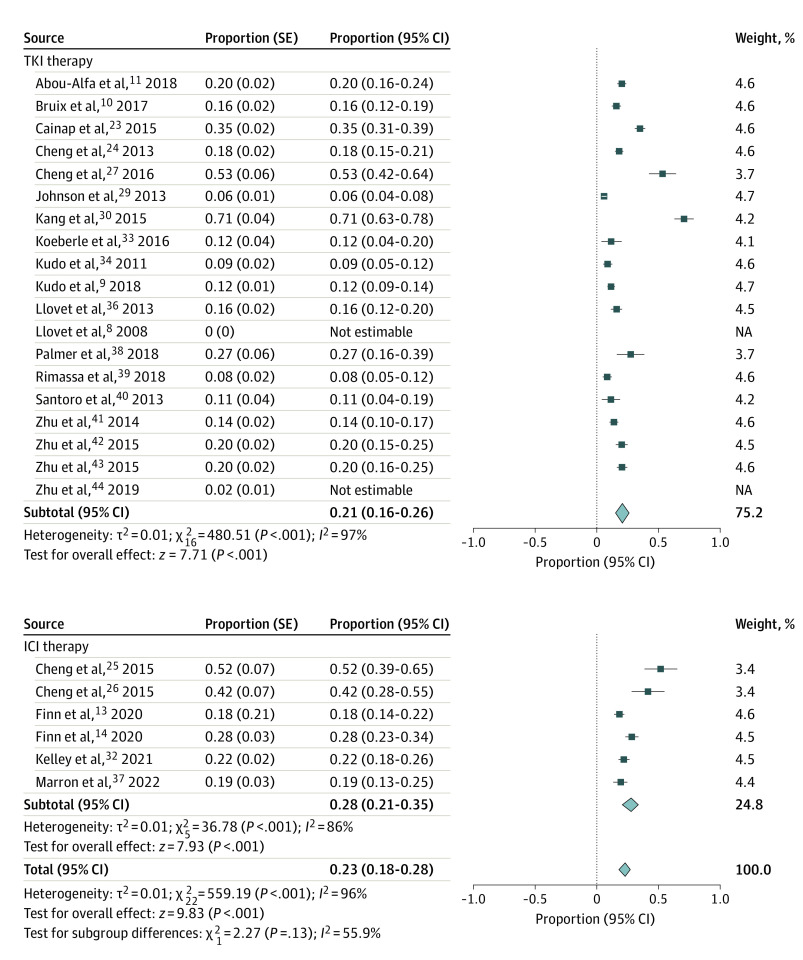
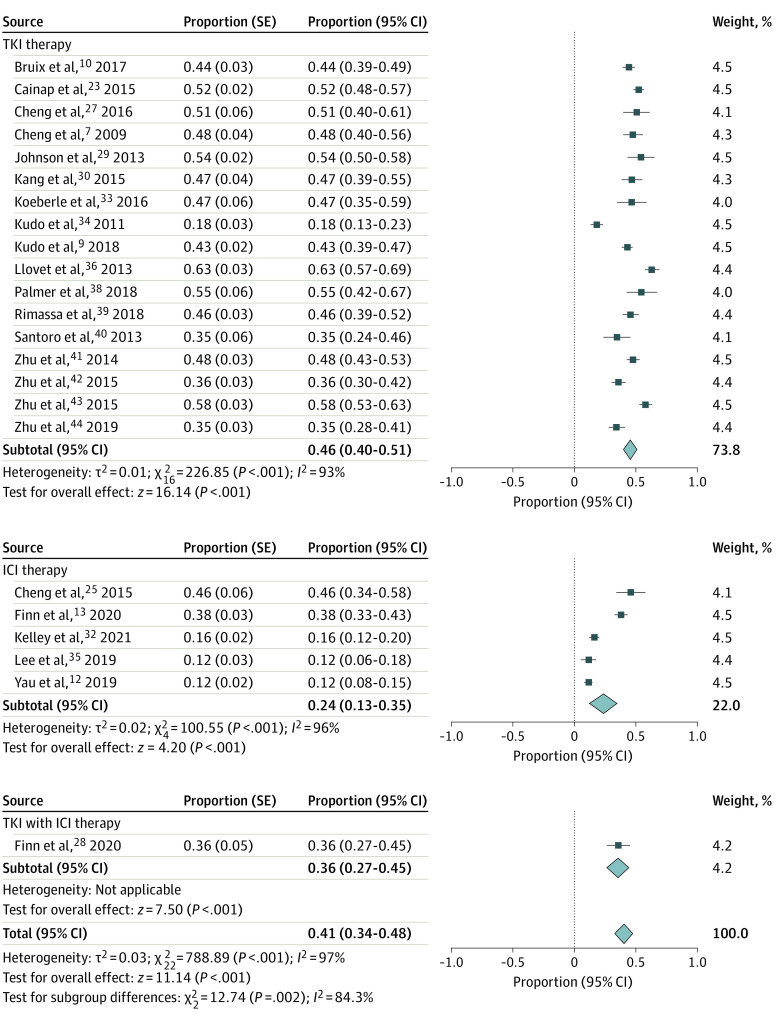
The primary outcome was the proportion of patients with clinically significant liver-related adverse events. Secondary outcomes included the proportion of patients who experienced clinically relevant (grade 3 or higher) adverse events and significant adverse events (ie, those that were life threatening, required hospitalization, or prolonged disability) as well as the risk ratio (RR) of these complications.
Overall, 30 studies with 12 921 patients were included. Patients had a mean (range) age of 62 (18-89) years; a mean (SD) 84% (3) were male; a mean (SD) 82% (16) had Barcelona Clinic Liver Cancer stage C HCC; and a mean (SD) 97% (6) had Childs A cirrhosis. Overall, 21% (95% CI, 16%-26%) of patients receiving TKIs had liver toxic effects compared with 28% (95% CI, 21%-35%) of patients receiving ICIs. Severe adverse events occurred in 46% (95% CI, 40%-51%) of patients receiving TKIs compared with 24% (95% CI, 13%-35%) of patients receiving ICIs. Compared with patients receiving sorafenib, other TKIs were associated with similar rates of liver toxic effects (RR, 1.06; 95% CI, 0.92-1.24) but higher rates of severe adverse events (RR, 1.24; 95% CI, 1.07-1.44). Comparing ICIs with sorafenib, there were similar rates of liver toxic effects (RR, 1.10; 95% CI, 0.86-1.40) and severe adverse events (RR, 1.19; 95% CI, 0.95-1.50).
In this systematic review and meta-analysis, serious adverse events were lower with ICIs than with TKIs, while liver toxic effects were similar. Combination therapy with novel ICIs is an appealing option in trials of neoadjuvant therapy for patients with HCC, requiring evaluation in preoperative trials.
最近靶向治疗和免疫疗法的发展使得新辅助治疗成为肝细胞癌(HCC)患者的一个有吸引力的选择。然而,外科医生担心这些药物的新辅助治疗的不良反应可能导致手术延迟甚至取消。
总结目前关于 HCC 患者使用酪氨酸激酶抑制剂(TKI)和免疫检查点抑制剂(ICI)的毒性谱的证据。
从 1990 年 1 月到 2021 年 12 月,对 Medline、Embase 和 Cochrane 中央对照试验注册中心(CENTRAL)进行了搜索。
符合纳入标准的单组、安慰剂对照和双药临床试验比较了 HCC 患者的 TKI 和 ICI。
根据系统评价和荟萃分析的首选报告项目指南,两名审查员独立提取数据。使用随机效应模型。
主要结局是具有临床意义的肝相关不良事件患者的比例。次要结局包括经历临床相关(3 级或更高)不良事件和显著不良事件(即危及生命、需要住院或延长残疾)的患者比例,以及这些并发症的风险比(RR)。
共有 30 项研究纳入了 12921 名患者。患者的平均(范围)年龄为 62(18-89)岁;平均(SD)84%(3)为男性;平均(SD)82%(16)为巴塞罗那临床肝癌 C 期 HCC;平均(SD)97%(6)为 Childs A 肝硬化。总体而言,21%(95%CI,16%-26%)接受 TKI 治疗的患者出现肝脏毒性反应,而 28%(95%CI,21%-35%)接受 ICI 治疗的患者出现肝脏毒性反应。接受 TKI 治疗的患者发生严重不良事件的比例为 46%(95%CI,40%-51%),而接受 ICI 治疗的患者为 24%(95%CI,13%-35%)。与接受索拉非尼的患者相比,其他 TKI 与相似的肝脏毒性反应率相关(RR,1.06;95%CI,0.92-1.24),但严重不良事件发生率较高(RR,1.24;95%CI,1.07-1.44)。与索拉非尼相比,ICI 与相似的肝脏毒性反应率(RR,1.10;95%CI,0.86-1.40)和严重不良事件率(RR,1.19;95%CI,0.95-1.50)相关。
在这项系统评价和荟萃分析中,ICI 治疗的严重不良事件低于 TKI 治疗,而肝脏毒性反应相似。新型 ICI 的联合治疗是 HCC 患者新辅助治疗试验中一个有吸引力的选择,需要在术前试验中进行评估。