Department of Medicine, Division of Nephrology, Toronto General Hospital (Y.L., V.L., J.T., L.C., D.Z.I.C.).
Temerty Faculty of Medicine (Y.L.).
Circulation. 2022 Aug 9;146(6):450-462. doi: 10.1161/CIRCULATIONAHA.122.059150. Epub 2022 Jul 11.
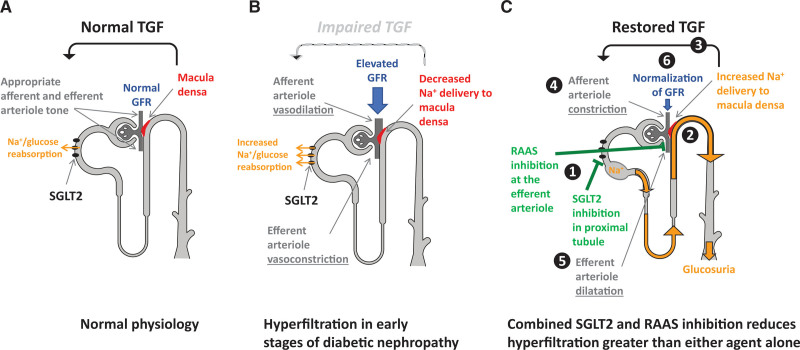
The cardiorenal effects of sodium-glucose cotransporter 2 inhibition (empagliflozin 25 mg QD) combined with angiotensin-converting enzyme inhibition (ramipril 10 mg QD) were assessed in this mechanistic study in patients with type 1 diabetes with potential renal hyperfiltration.
Thirty patients (out of 31 randomized) completed this double-blind, placebo-controlled, crossover trial. Recruitment was stopped early because of an unexpectedly low proportion of patients with hyperfiltration. Measurements were obtained after each of the 6 treatment phases over 19 weeks: (1) baseline without treatment, (2) 4-week run-in with ramipril treatment alone, (3) 4-week combined empagliflozin-ramipril treatment, (4) a 4-week washout, (5) 4-week combined placebo-ramipril treatment, and (6) 1-week follow-up. The primary end point was glomerular filtration rate (GFR) after combination treatment with empagliflozin-ramipril compared with placebo-ramipril. GFR was corrected for ramipril treatment alone before randomization. At the end of study phase, the following outcomes were measured under clamped euglycemia (4 to 6 mmol/L): inulin (GFR) and para-aminohippurate (effective renal plasma flow) clearances, tubular sodium handling, ambulatory blood pressure, arterial stiffness, heart rate variability, noninvasive cardiac output monitoring, plasma and urine biochemistry, markers of the renin-angiotensin-aldosterone system, and oxidative stress.
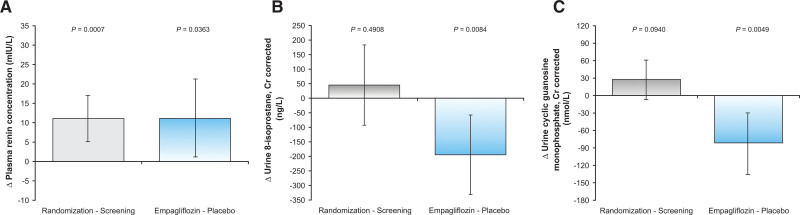
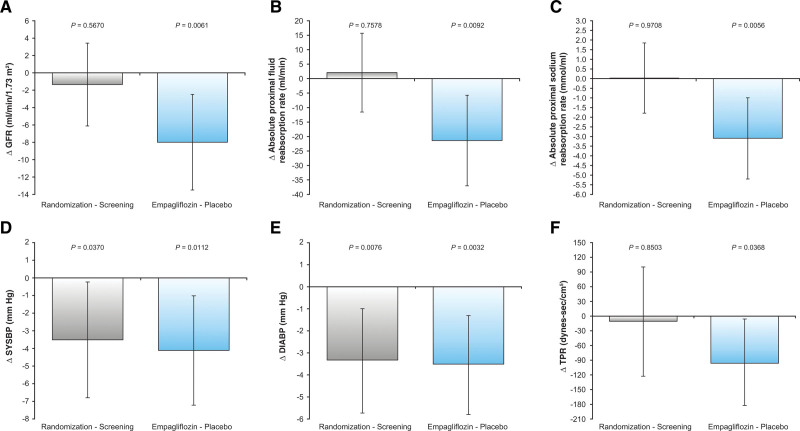
Combination treatment with empagliflozin-ramipril resulted in an 8 mL/min/1.73 m lower GFR compared with placebo-ramipril treatment (=0.0061) without significant changes to effective renal plasma flow. GFR decrease was accompanied by a 21.3 mL/min lower absolute proximal fluid reabsorption rate (=0.0092), a 3.1 mmol/min lower absolute proximal sodium reabsorption rate (=0.0056), and a 194 ng/mmol creatinine lower urinary 8-isoprostane level (=0.0084) relative to placebo-ramipril combination treatment. Sodium-glucose cotransporter 2 inhibitor/angiotensin-converting enzyme inhibitor combination treatment resulted in additive blood pressure-lowering effects (clinic systolic blood pressure lower by 4 mm Hg [=0.0112]; diastolic blood pressure lower by 3 mm Hg [=0.0032]) in conjunction with a 94.5 dynes × sex/cm lower total peripheral resistance (=0.0368). There were no significant changes observed to ambulatory blood pressure, arterial stiffness, heart rate variability, or cardiac output with the addition of empagliflozin.
Adding sodium-glucose cotransporter 2 inhibitor treatment to angiotensin-converting enzyme inhibitor resulted in an expected GFR dip, suppression of oxidative stress markers, additive declines in blood pressure and total peripheral resistance. These changes are consistent with a protective physiologic profile characterized by the lowering of intraglomerular pressure and related cardiorenal risk when adding a sodium-glucose cotransporter 2 inhibitor to conservative therapy.
URL: https://www.
gov; Unique identifier: NCT02632747.
本机制研究评估了钠-葡萄糖共转运蛋白 2 抑制剂(恩格列净 25mgQD)联合血管紧张素转换酶抑制剂(雷米普利 10mgQD)在伴有潜在肾功能超滤的 1 型糖尿病患者中的心脏肾脏作用。
31 例随机患者中,有 30 例完成了这项双盲、安慰剂对照、交叉试验。由于超滤患者的比例出乎意料地低,提前停止了招募。在 19 周的 6 个治疗阶段中,每个阶段都获得了以下测量值:(1)无治疗的基线,(2)单独使用雷米普利的 4 周导入期,(3)恩格列净-雷米普利联合治疗的 4 周,(4)4 周洗脱期,(5)联合安慰剂-雷米普利治疗的 4 周,以及(6)1 周随访。主要终点是与安慰剂-雷米普利相比,恩格列净-雷米普利联合治疗后的肾小球滤过率(GFR)。在随机分组前,GFR 经过雷米普利单独治疗校正。在研究阶段结束时,在夹闭性血糖(4 至 6mmol/L)下测量了以下结果:菊粉(GFR)和对氨基马尿酸(有效肾血浆流量)清除率、肾小管钠处理、动态血压、动脉僵硬度、心率变异性、无创心输出量监测、血浆和尿液生化、肾素-血管紧张素-醛固酮系统标志物和氧化应激。
与安慰剂-雷米普利联合治疗相比,恩格列净-雷米普利联合治疗导致 GFR 降低 8mL/min/1.73m(=0.0061),而有效肾血浆流量无显著变化。GFR 下降伴随着绝对近端液体重吸收率降低 21.3mL/min(=0.0092)、绝对近端钠吸收率降低 3.1mmol/min(=0.0056)和尿 8-异前列腺素水平降低 194ng/mmol 肌酐(=0.0084)与安慰剂-雷米普利联合治疗相比。钠-葡萄糖共转运蛋白 2 抑制剂/血管紧张素转换酶抑制剂联合治疗在降低诊室收缩压 4mmHg(=0.0112)和舒张压 3mmHg(=0.0032)方面具有相加的降压作用,同时总外周阻力降低 94.5 dynes × sex/cm(=0.0368)。添加恩格列净后,动态血压、动脉僵硬度、心率变异性或心输出量均无明显变化。
在血管紧张素转换酶抑制剂的基础上加用钠-葡萄糖共转运蛋白 2 抑制剂治疗,导致预期的 GFR 下降,氧化应激标志物得到抑制,血压和总外周阻力进一步下降。这些变化与一种保护生理特征一致,即在保守治疗中加用钠-葡萄糖共转运蛋白 2 抑制剂可降低肾小球内压和相关的心肾风险。
网址:https://www.
gov;独特标识符:NCT02632747。