Department of Anesthesiology, The General Hospital of Western Theater Command, Sichuan, China.
Department of Anesthesiology, No. 950 Hospital of PLA, Yecheng, China.
Medicine (Baltimore). 2022 Jul 22;101(29):e29584. doi: 10.1097/MD.0000000000029584.
Opioid-induced nausea and vomiting are common side effects of patient-controlled intravenous analgesia (PCIA). This study aimed to explore the inhibitory effect of a naloxone admixture on the incidence of sufentanil-induced postoperative nausea and vomiting (PONV).
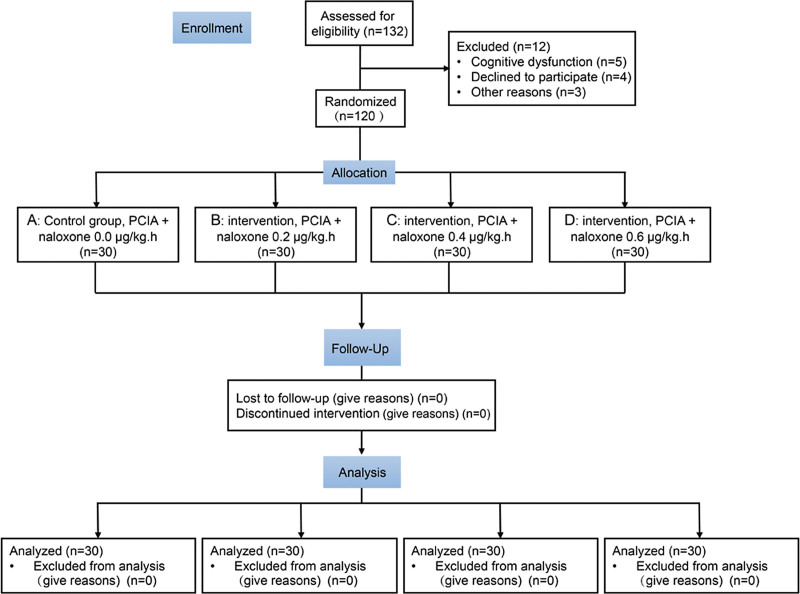
A total of 132 Uyghur American Society of Anesthesiologists I and II patients scheduled to undergo elective gynecological laparoscopic surgery were recruited; among these, 120 patients were enrolled and randomly allocated into 4 groups: patients receiving PCIA but no naloxone were included in the control group (group A); patients receiving PCIA with a low-dose naloxone admixture at 0.2 μg·kg-1·h-1 were included in group B; patients receiving PCIA with naloxone admixture at 0.4 μg·kg-1·h-1 were included in group C; patients receiving PCIA with naloxone admixture at 0.6 μg·kg-1·h-1 were included in group D. All patients were administered sufentanil at 0.04 kg-1·h-1, butorphanol at 2 kg-1·h-1, and dexmedetomidine at 0.08 kg-1·h-1 using a PCIA device within 2 days of surgery. The occurrence of nausea and vomiting, visual analogue scores for pain intensity, mean arterial pressure, heart rate, oxygen saturation, pruritus, lethargy, respiratory depression, etc, was recorded at 2, 8, 12, 24, and 48 hours postoperatively.
There was a significant difference in the PONV scores between the groups at 8, 12, and 24 hours after surgery (P < 0.01). At 8 and 12 hours, the score of group C/D was significantly lower than that of group A/B (P < 0.01). At 24 hours after surgery, the PONV score of group B/C/D was significantly lower than that of group A (P < 0.01). No significant difference was observed in the general data and visual analogue scores for postoperative pain between the 4 groups.
Naloxone admixture administered at 0.4 to 0.6 μg·kg-1·h-1 can exert an effective inhibitory effect on the incidence and intensity of PONV in gynecological laparoscopic surgery.
阿片类药物引起的恶心和呕吐是患者自控静脉镇痛(PCIA)的常见副作用。本研究旨在探讨纳洛酮混合物对舒芬太尼引起的术后恶心和呕吐(PONV)发生率的抑制作用。
共纳入 132 例维吾尔族美国麻醉医师协会 I 级和 II 级择期妇科腹腔镜手术患者;其中 120 例患者被纳入并随机分为 4 组:接受 PCIA 但不接受纳洛酮的患者纳入对照组(A 组);接受 PCIA 并以 0.2μg·kg-1·h-1 的低剂量纳洛酮混合物的患者纳入 B 组;接受 PCIA 并以 0.4μg·kg-1·h-1 的纳洛酮混合物的患者纳入 C 组;接受 PCIA 并以 0.6μg·kg-1·h-1 的纳洛酮混合物的患者纳入 D 组。所有患者在手术后 2 天内均使用 PCIA 设备以 0.04μg·kg-1·h-1 的舒芬太尼、2μg·kg-1·h-1 的布托啡诺和 0.08μg·kg-1·h-1 的右美托咪定进行治疗。记录术后 2、8、12、24 和 48 小时时恶心和呕吐的发生、疼痛强度的视觉模拟评分、平均动脉压、心率、血氧饱和度、瘙痒、昏睡、呼吸抑制等情况。
术后 8、12 和 24 小时,各组间 PONV 评分差异有统计学意义(P<0.01)。在 8 小时和 12 小时时,C 组/D 组的评分明显低于 A 组/B 组(P<0.01)。术后 24 小时时,B 组/C 组/D 组的 PONV 评分明显低于 A 组(P<0.01)。4 组患者的一般资料和术后疼痛视觉模拟评分差异无统计学意义。
在妇科腹腔镜手术中,0.4 至 0.6μg·kg-1·h-1 的纳洛酮混合物可以有效抑制 PONV 的发生率和强度。