Center for Acute Care Nephrology, Cincinnati Children's Hospital Medical Center, 3333 Burnet Avenue, MLC 7022, Cincinnati, Ohio, 45229, USA.
University of Michigan Medical Center, University of Michigan Hospital, Ann Arbor, MI, USA.
Pediatr Nephrol. 2023 Mar;38(3):927-931. doi: 10.1007/s00467-022-05692-1. Epub 2022 Jul 23.
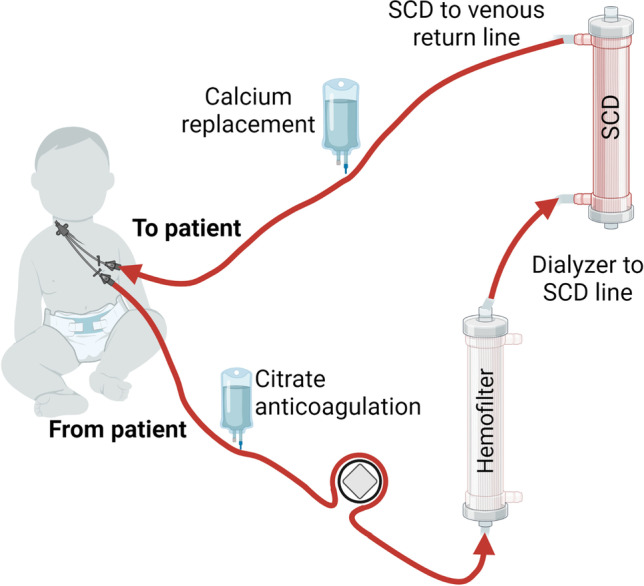
Hemophagocytic lymphohistiocytosis (HLH) is a dysregulated immune disorder in children, associated with Epstein-Barr virus (EBV) infection or malignancies. In severe forms, HLH presents with signs and symptoms of hyperinflammation that progress to life-threatening multiorgan failure. Intervention with an extracorporeal immunomodulatory treatment utilizing a selective cytopheretic device (SCD) could be beneficial. The SCD with regional citrate anticoagulation selectively binds the most highly activated circulating neutrophils and monocytes and deactivates them before release to the systemic circulation. Multiple clinical studies, including a multicenter study in children, demonstrate SCD therapy attenuates hyperinflammation, resolves ongoing tissue injury and allows progression to functional organ recovery. We report the first case of SCD therapy in a patient with HLH and multi-organ failure.
CASE DIAGNOSIS/TREATMENT: A previously healthy 22-month-old toddler presented with fever, abdominal distension, organomegaly, pancytopenia, and signs of hyperinflammation. EBV PCR returned at > 25 million copies. The clinical and laboratory pictures were consistent with systemic EBV-positive T-cell lymphoma with symptoms secondary to HLH. The patient met inclusion criteria for an ongoing study of integration of the SCD with a continuous kidney replacement therapy (CKRT) as part of standard of care. The patient received CKRT-SCD for 4 days with normalization of serum markers of sepsis and inflammation. The patient underwent hematopoietic stem cell transplantation 52 days after presentation and has engrafted with normal kidney function 8 months later.
SCD treatment resulted in improvement of poor tissue perfusion reflected by rapid decline in serum lactate levels, lessened systemic capillary leak with discontinuation of vasoactive agents, and repair and recovery of lung and kidney function with extubation and removal of hemodialysis support.
噬血细胞性淋巴组织细胞增生症(HLH)是一种儿童中失调的免疫性疾病,与 EBV 感染或恶性肿瘤有关。在严重的情况下,HLH 表现出炎症过度活跃的迹象和症状,进而导致危及生命的多器官衰竭。采用体外免疫调节治疗方法,利用选择性细胞分离装置(SCD)可能会有所帮助。采用局部枸橼酸盐抗凝的 SCD 选择性地结合最活跃的循环中性粒细胞和单核细胞,并在它们释放到全身循环之前使它们失活。多项临床研究,包括一项儿童多中心研究,表明 SCD 治疗可减轻炎症过度活跃,解决持续的组织损伤,并使器官功能恢复。我们报告了首例 HLH 伴多器官衰竭患者使用 SCD 治疗的病例。
病例诊断/治疗:一名先前健康的 22 个月大的幼儿出现发热、腹胀、器官肿大、全血细胞减少和炎症过度活跃的迹象。EBV PCR 结果为>2500 万拷贝。临床表现和实验室检查结果与全身 EBV 阳性 T 细胞淋巴瘤一致,症状继发于 HLH。该患者符合正在进行的 SCD 与连续肾脏替代治疗(CKRT)整合的研究纳入标准,作为标准治疗的一部分。该患者接受 CKRT-SCD 治疗 4 天,血清败血症和炎症标志物恢复正常。该患者在发病后 52 天接受造血干细胞移植,8 个月后肾功能正常。
SCD 治疗导致组织灌注不良的改善,反映在血清乳酸水平的迅速下降;停用血管活性药物后,全身毛细血管渗漏减少;肺和肾功能的修复和恢复,成功撤机并停用血液透析支持。