Klötzsch Christof, Böhmert Matthias, Hermann Ruxandra, Teegen Bianca, Rentzsch Kristin, Till Andreas
Department of Neurology, Hegau-Bodensee-Hospital, Virchowstrasse 10, 78224, Singen, Germany.
Clinical Immunological Laboratory Prof. Dr. Med. Winfried Stöcker, Seekamp 31, 23560, Lübeck, Germany.
Neurol Res Pract. 2022 Jul 25;4(1):29. doi: 10.1186/s42466-022-00194-9.
Subacute cerebellar ataxia combined with cerebrospinal fluid (CSF) pleocytosis is the result of an immune response that can occur due to viral infections, paraneoplastic diseases or autoimmune-mediated mechanisms. In the following we present the first description of a patient with anti-Homer-3 antibodies in serum and CSF who has been diagnosed with paraneoplastic subacute cerebellar degeneration due to a papillary adenocarcinoma of the breast.
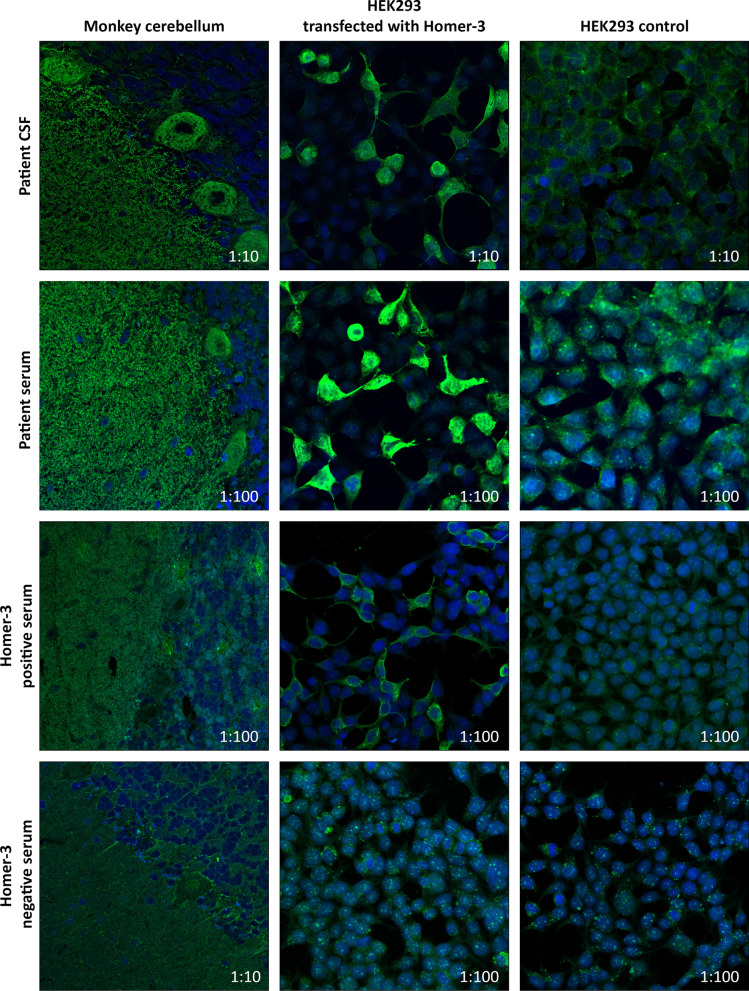
A 58-year-old female was admitted to our clinical department because of increasing gait and visual disturbances starting nine months ago. The neurological examination revealed a downbeat nystagmus, oscillopsia, a severe standing and gait ataxia and a slight dysarthria. Cranial MRI showed no pathological findings. Examination of CSF showed a lymphocytic pleocytosis of 11 cells/µl and an intrathecal IgG synthesis of 26%. Initially, standard serological testing in serum and CSF did not indicate any autoimmune or paraneoplastic aetiology. However, an antigen-specific indirect immunofluorescence test (IIFT) revealed the presence of anti-Homer-3 antibodies (IgG) with a serum titer of 1: 32,000 and a titer of 1: 100 in CSF. Subsequent histological examination of a right axillary lymph node mass showed papillary adenocarcinoma cells. Breast MRI detected multiple bilateral lesions as a diffuse tumour manifestation indicative of adenocarcinoma of the breast. Treatment with high-dose methylprednisolone followed by five plasmaphereses and treatment with 4-aminopyridine resulted in a moderate decrease of the downbeat nystagmus and she was able to move independently with a wheeled walker after 3 weeks. The patient was subsequently treated with chemotherapy (epirubicin, cyclophosphamide) and two series of immunoglobulins (5 × 30 g each). This resulted in a moderate improvement of the cerebellar symptoms with a decrease of ataxia and disappearance of the downbeat nystagmus.
The presented case of anti-Homer-3 antibody-associated cerebellar degeneration is the first that is clearly associated with the detection of a tumour. Interestingly, the Homer-3 protein interaction partner metabotropic glutamate receptor subtype 1A (mGluR1A) is predominantly expressed in Purkinje cells where its function is essential for motor coordination and motor learning. Based on our findings, in subacute cerebellar degeneration, we recommend considering serological testing for anti-Homer-3 antibodies in serum and cerebrospinal fluid together with tumor screening.
亚急性小脑性共济失调合并脑脊液(CSF)细胞增多是一种免疫反应的结果,可由病毒感染、副肿瘤性疾病或自身免疫介导机制引起。以下我们首次描述了一名血清和脑脊液中存在抗Homer-3抗体的患者,该患者因乳腺乳头状腺癌被诊断为副肿瘤性亚急性小脑变性。
一名58岁女性因9个月前开始出现步态和视觉障碍加重而入住我院临床科室。神经系统检查发现下跳性眼球震颤、视振荡、严重的站立和步态共济失调以及轻度构音障碍。头颅MRI未发现病理改变。脑脊液检查显示淋巴细胞增多,为11个细胞/微升,鞘内IgG合成率为26%。最初,血清和脑脊液中的标准血清学检测未显示任何自身免疫或副肿瘤病因。然而,一项抗原特异性间接免疫荧光试验(IIFT)显示血清中抗Homer-3抗体(IgG)滴度为1:32,000,脑脊液中滴度为1:100。随后对右侧腋窝淋巴结肿块进行组织学检查,发现乳头状腺癌细胞。乳腺MRI检测到多个双侧病变,表现为弥漫性肿瘤,提示乳腺腺癌。大剂量甲泼尼龙治疗,随后进行5次血浆置换,并使用4-氨基吡啶治疗,使下跳性眼球震颤中度减轻,3周后她能够借助轮式助行器独立行走。该患者随后接受了化疗(表柔比星、环磷酰胺)和两系列免疫球蛋白治疗(每次5×30g)。这使小脑症状得到中度改善,共济失调减轻,下跳性眼球震颤消失。
所呈现的抗Homer-3抗体相关小脑变性病例是首例与肿瘤检测明确相关的病例。有趣的是,Homer-3蛋白相互作用伙伴代谢型谷氨酸受体亚型1A(mGluR1A)主要在浦肯野细胞中表达,其功能对运动协调和运动学习至关重要。基于我们的发现,对于亚急性小脑变性,我们建议考虑检测血清和脑脊液中的抗Homer-3抗体,并进行肿瘤筛查。